
High-Risk Surgery Denied Due to Diabetes, Heart Disease, or Obesity? A Beijing MDT Pathway for Complex Surgical Cases
SEO Title: High-Risk Surgery Denied? Beijing MDT Options for Diabetes and Heart Disease
You were told the surgery is too risky. Maybe it was delayed. Maybe it was declined outright. For many patients with diabetes, heart disease, or severe obesity, the issue is not always the operation itself. It is whether the hospital is willing to manage the risk around it.
In Beijing, top Grade-3A hospitals handle complex surgical patients at a scale most systems do not. That matters when your case has already been labeled “too high risk.”
TL;DR: Decision Summary
| Factor | Typical Western Pathway | Beijing Top Grade-3A MDT Pathway |
|---|---|---|
| First-line treatment | Delay surgery until risk factors improve, or decline the case if perioperative risk is judged too high. | Use an MDT review to decide whether the risk can be actively optimized before surgery. |
| Specialist wait time | Often takes weeks to months to coordinate across multiple specialties. | Internal MDT coordination is often faster once the case is accepted for review. |
| Out-of-pocket cost | Can be high and unpredictable, especially in private systems. | Case-dependent. Usually discussed after records review and department acceptance. |
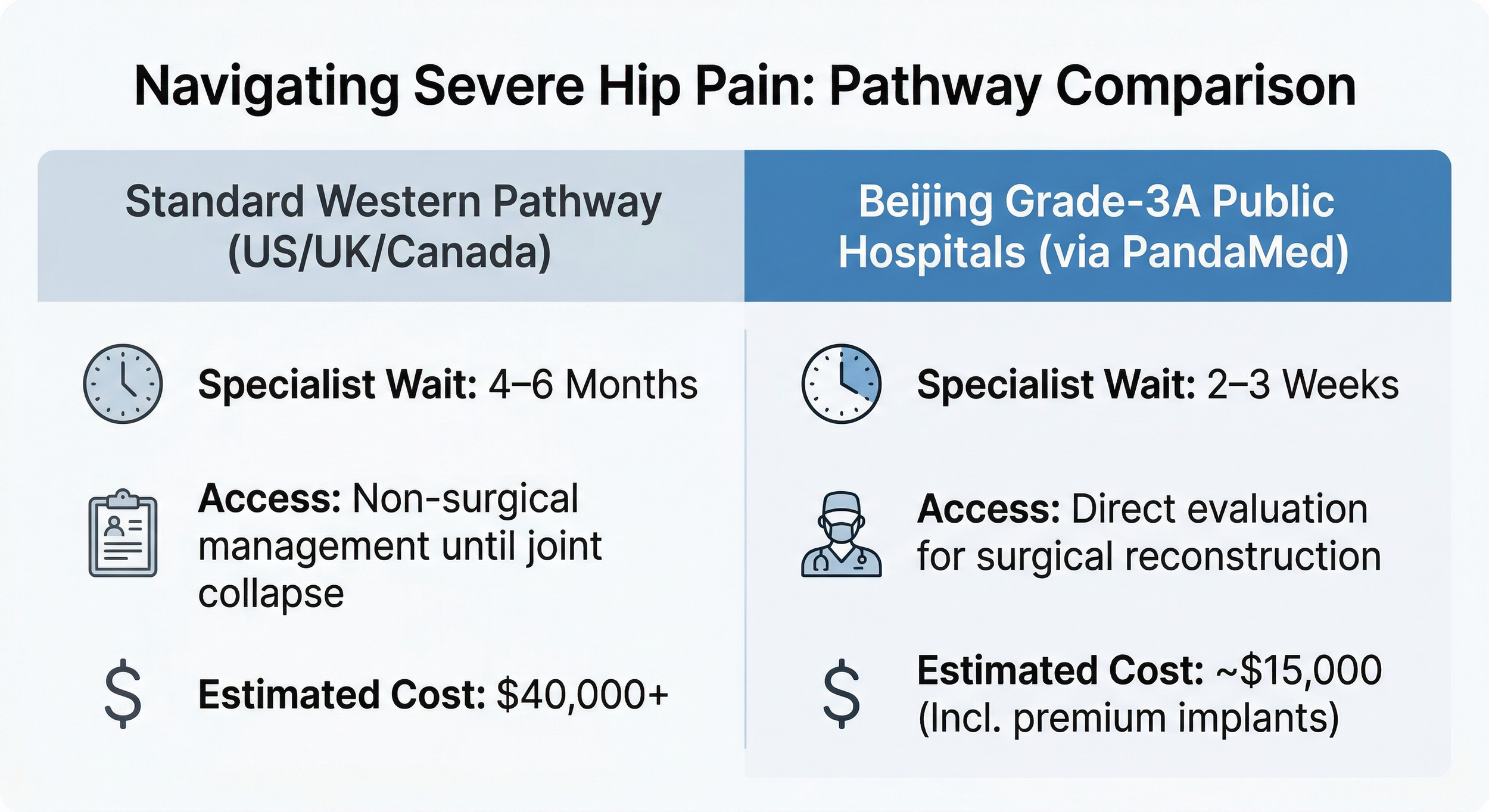
Figure 1 - Comparison of typical localized surgical denial pathways versus the Beijing active MDT assessment approach.
Why You Cannot Just “Wait and See”
Variable 1: The comorbidity stack changes surgical risk fast
This is the part many patients never get fully explained. A single risk factor is one thing. A stack of risk factors is another.
Patients with diabetic-range preoperative glucose going into major noncardiac surgery have been reported to face a 4.0x higher risk of cardiovascular-related death versus patients without that issue. Patients with overlapping cardiovascular risk factors, including diabetes and hypertension, have shown an adjusted 5.54x higher risk of perioperative myocardial infarction in noncardiac surgery settings.
That is why many hospitals hesitate. They are not only thinking about the surgeon’s skill. They are thinking about anesthesia stress, blood pressure swings, glucose instability, cardiac reserve, and ICU backup.
Top Beijing centers approach this differently. In hospitals such as PUMCH and Beijing Anzhen Hospital, these variables are not treated as an automatic stop sign. They are treated as perioperative control targets. High-volume teams see more unstable patients, more edge cases, and more rescue scenarios. That kind of repetition improves precision.
Variable 2: Infection and healing risk can block otherwise necessary surgery
Diabetes does not just affect sugar. It affects wound healing, infection risk, and recovery speed.
A multicenter matched study found that diabetic patients undergoing major surgery had markedly higher odds of severe postoperative infectious complications, including necrotizing fasciitis at 3.98x and pyogenic arthritis at 3.89x compared with non-diabetic patients.
This is one reason some systems push delay after delay. If a hospital expects poor healing, readmission risk, or prolonged antibiotic care, it may decide the case is operationally unattractive before it is medically impossible.
Beijing MDT teams often intervene before the operation starts. Endocrinology works on glucose control. Cardiology assesses tolerance to hemodynamic stress. Anesthesiology plans around instability, not around a best-case scenario. That is the difference between passive waiting and active optimization.
Variable 3: Recovery time and ICU demand affect hospital willingness to accept the case
Many patients think the rejection is only about safety. In reality, recovery burden matters too.
Published data in cardiac surgical populations shows that patients with diabetes and cardiovascular comorbidity can have longer hospital stays, with one cited comparison showing an increase from 6.0 to 9.6 days, or about 60% longer. Other studies also show higher complication load and worse overall outcomes in diabetic cardiac patients.
Hospitals with tighter ICU capacity and stricter bed turnover pressure may be less willing to take on these cases. That does not mean surgery is always impossible. It may mean the local system is not built for high-friction recovery.
In Beijing, major public hospitals were built around high patient throughput and specialty concentration. In complex surgical pathways, that system can support tighter post-op monitoring, faster specialty response, and more coordinated rescue if recovery stalls.
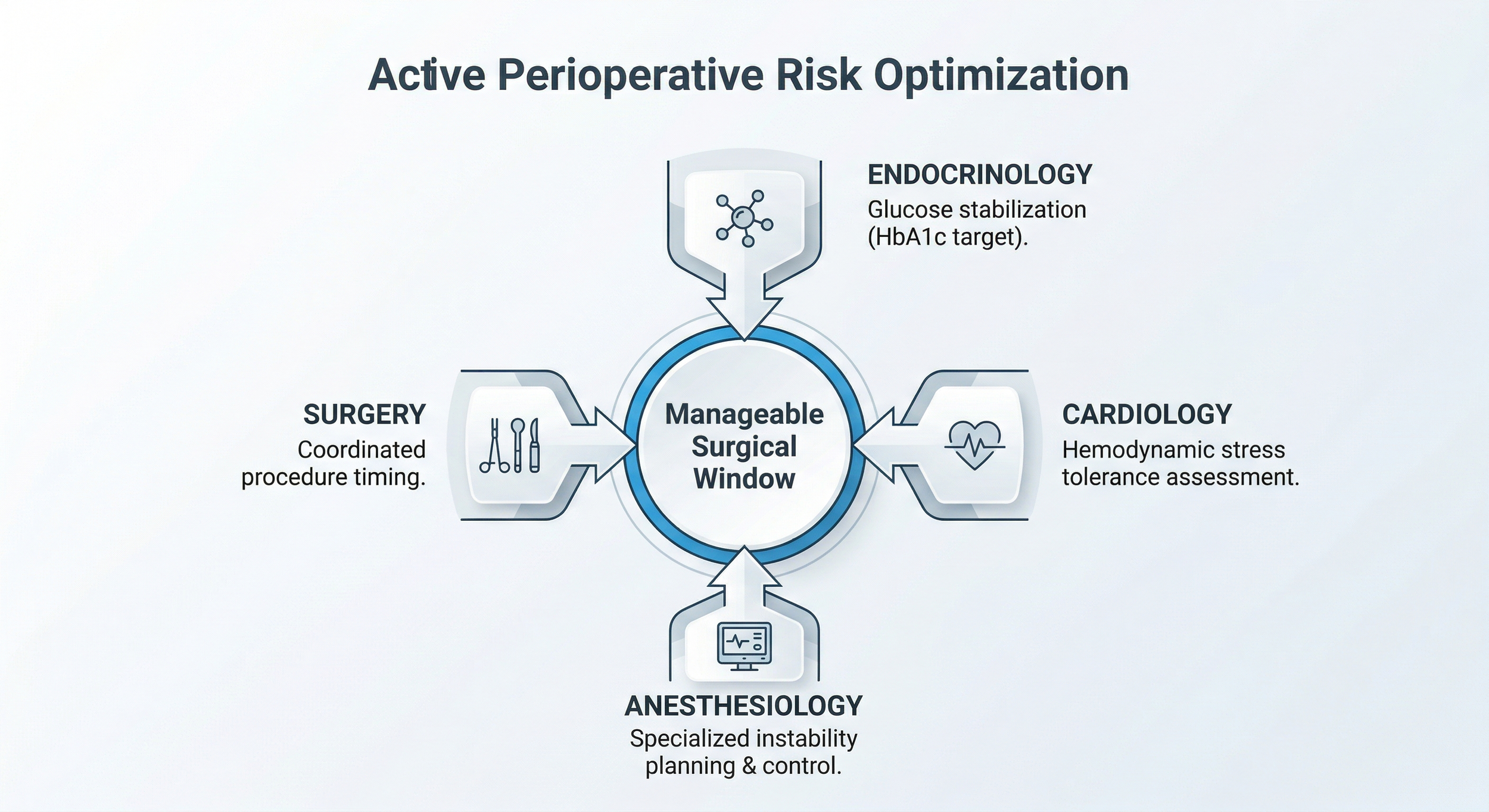
Figure 2 - Conceptual diagram of how different medical specialties coordinate in Beijing to actively optimize high-risk comorbidities before surgery.
Beijing MDT Strength: What the Team Actually Does
At the top level, this is not “a good surgeon plus luck.” It is coordinated risk control.
Endocrinology works to bring glucose into a safer range before the operation.
Cardiology checks whether the heart can tolerate anesthesia, bleeding shifts, and fluid changes.
Anesthesiology is often the deciding specialty in a high-risk case. The anesthesia plan can determine whether a patient stays stable during a long operation.
Surgery then proceeds only after the risk window is judged manageable, not ideal.
At centers like PUMCH, complex systemic disease is part of daily tertiary referral care. At Anzhen, cardiovascular complexity is a core strength. That kind of concentration matters when your risk profile already scared off other hospitals.
Beijing Hospital and Surgeon Profiles
PUMCH (Peking Union Medical College Hospital) is one of the most recognized top-tier public hospitals in China. It is known for handling difficult referral cases, complex internal medicine overlap, and high-level multidisciplinary coordination across departments.
Beijing Anzhen Hospital is one of China’s strongest names in cardiovascular care. For surgical candidates with serious heart history, it is one of the most important referral anchors in Beijing.
Dr. J is a Chief Physician with 20+ years in complex perioperative management. He works on patients with unstable metabolic and cardiovascular profiles and has participated in 1,000+ high-complexity surgical cases per year within a tertiary referral setting.
Dr. Z is a senior Professor-level anesthesiology expert with 20+ years of experience in high-risk operations. His focus is intraoperative hemodynamic control in patients other teams may classify as borderline operable.
Figure 3 - Illustrative concept of Chief Physicians and specialists collaborating in a high-volume Beijing Grade-3A hospital setting for complex case review.
Stop Guessing
Stop guessing. Let a Beijing Chief Surgeon review your actual MRI scans, CT images, lab results, and medical history. Specialist Case Review gives you a structured, objective surgical plan translated into English.
A Realistic Case Example
A 65-year-old UK patient needed colon tumor surgery. He also had a BMI of 39, HbA1c of 9.4%, and a history of two coronary stents. His local options were delayed or declined because the combined operative risk was considered too high.
After record review, a Beijing MDT pathway was explored. His existing scans and reports were translated and reformatted for specialist review. Before surgery, the team focused on short-term metabolic and cardiac stabilization. Once his numbers reached a workable range, a senior anesthesia-led plan supported the operation. He completed surgery and entered recovery with close monitoring.
This type of case does not mean every denied patient can be accepted. It means some patients need a system that is built to assess complexity instead of rejecting it at first pass.
The Checklist: What to Send for an Initial Review
You do not need brand-new tests just to start.
Have old scans? That’s fine for an initial look. Existing records are usually enough for triage.
Please send whatever you already have:
Most recent diagnosis summary
Surgical recommendation or rejection note, if available
CT, MRI, PET-CT, or X-ray reports
Pathology report, if relevant
Recent blood tests
HbA1c, fasting glucose, or diabetes records
Cardiology records, ECG, echo, stent history, or stress test reports
Medication list
Past surgery history
If something is missing, the first step is still the same: review the current file set and see whether Beijing specialists think the case is workable.
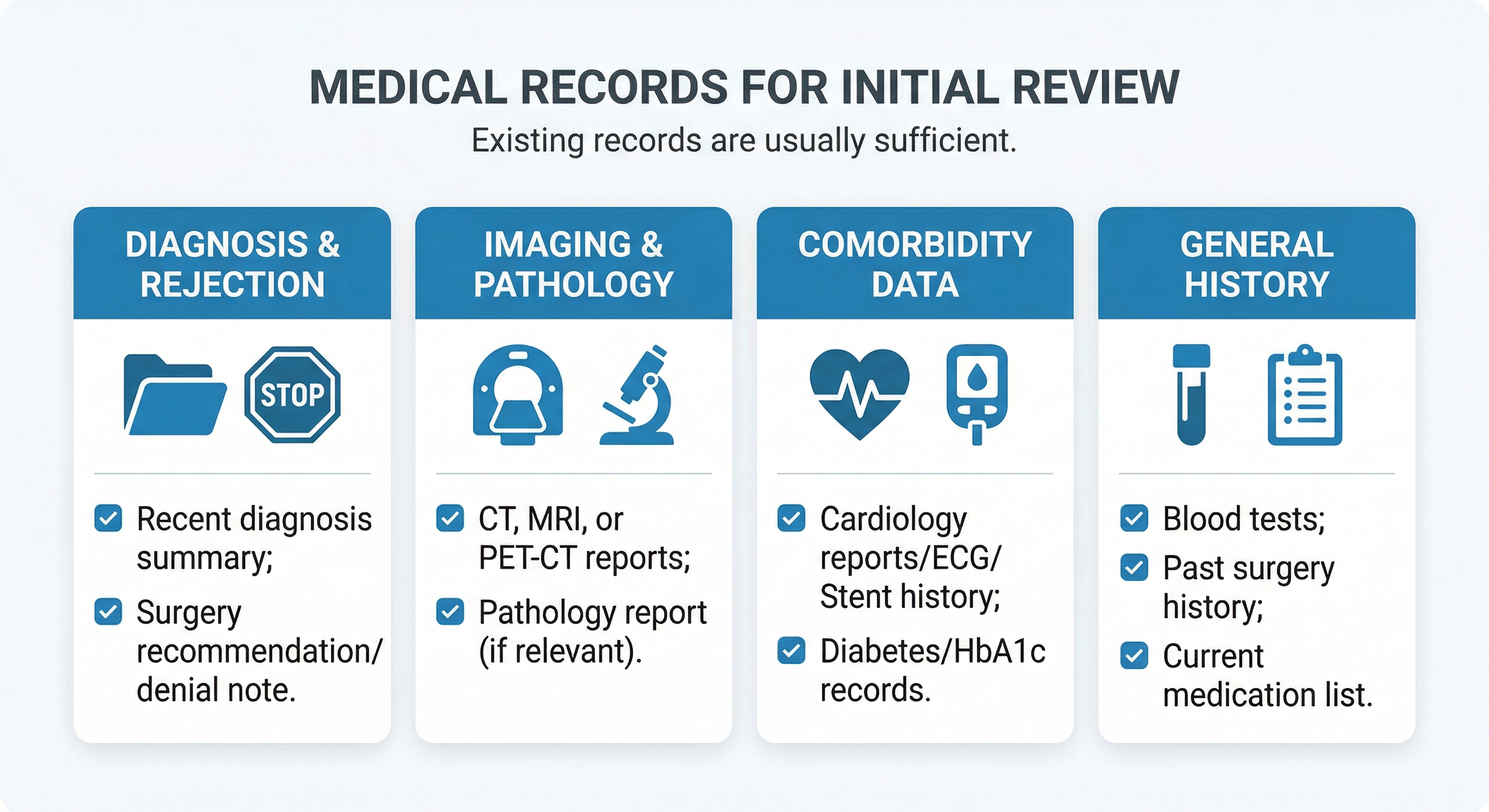
Figure 4 - Essential medical records checklist required for an initial specialist case review by Beijing MDT teams.
Author Bio
Ryan Lee is a Beijing-based medical concierge and the founder of PandaMed. With a strict compliance background, he helps international patients navigate China's top public hospitals safely. He secures direct access to Chief Physicians for complex cases.
Medical Disclaimer
This information is for educational purposes only and is not medical advice. PandaMed is a care coordination service, not a medical provider. Always consult a qualified doctor for your specific condition.
References
Noordzij PG, et al. Increased preoperative glucose levels are associated with perioperative mortality in patients undergoing noncardiac, nonvascular surgery. European Journal of Endocrinology.
https://pubmed.ncbi.nlm.nih.gov/17164235/Wilcox T, et al. Cardiovascular Risk Factors and Perioperative Myocardial Infarction After Noncardiac Surgery. Canadian Journal of Cardiology.
https://pubmed.ncbi.nlm.nih.gov/32620387/Lin CS, et al. Adverse Outcomes after Major Surgeries in Patients with Diabetes: A Multicenter Matched Study. Journal of Clinical Medicine.
https://pubmed.ncbi.nlm.nih.gov/30626192/Raza S, et al. Coronary artery bypass grafting in diabetics: A growing health care cost crisis. The Journal of Thoracic and Cardiovascular Surgery.
https://pubmed.ncbi.nlm.nih.gov/25956269/Santos KA, et al. Prognosis and Complications of Diabetic Patients Undergoing Isolated Coronary Artery Bypass Surgery. Brazilian Journal of Cardiovascular Surgery.
https://pubmed.ncbi.nlm.nih.gov/27074277/
Internal source note: Surgical volume and tertiary referral complexity data for leading Beijing Grade-3A hospitals are cited as department-level background descriptions only, based on 2023 internal hospital reporting and public institutional standing.