
Severe Type 2 Diabetes and Obesity: When Medication Stops Working, Metabolic Surgery in Beijing Becomes the Next Step
SEO Title: Beyond Weight Loss: Reverse Type 2 Diabetes with Metabolic Surgery in Beijing
You followed the standard path. Pills first. Then more pills. Then insulin. Maybe now a costly GLP-1 shot every week.
But for many people with Type 2 diabetes and obesity, meds control numbers without stopping the long-term damage. Blood sugar may move. The disease still moves too. That is why more international patients are looking at metabolic surgery in Beijing as a serious treatment option, not just a weight-loss procedure.

Figure 1 - Visual overview: Transiting from standard medical therapy to metabolic surgery pathways in Beijing.
TL;DR: A Fast Comparison Before You Decide
This guide outlines the clinical pathways, long-term costs, and realistic timelines for international patients seeking to reverse severe Type 2 Diabetes and obesity through metabolic surgery in Beijing.
| Factor | Typical Western Pathway | Beijing Top Grade-3A MDT Pathway |
|---|---|---|
| First-line treatment | Delay surgery until risk factors improve, or decline case if perioperative risk is too high. | MDT review to decide whether risk can be actively optimized before surgery. |
| Specialist wait time | Often weeks to months for multi-specialty coordination. | Faster internal MDT coordination once case is accepted. |
| Out-of-pocket cost | $85,500 - $130,000+ | $12,000 - $18,000 (One-time cost) |
Don't wait months to find out if you need surgery. Get a clear answer on your eligibility first.
Why You Cannot Just “Wait and See”
Variable 1: The Main Threat Is Not Just High Blood Sugar. It Is Cardiovascular Damage.
Type 2 diabetes is not only a glucose problem. It is a full-body vascular disease. The biggest long-term threat is often heart attack, stroke, heart failure, and other cardiovascular complications.
The data is blunt. Cardiovascular disease is the leading cause of death in people with Type 2 diabetes. Globally, about 50.3% of patients with T2D ultimately die from cardiovascular complications. Compared with adults without diabetes, people with T2D face about 2 to 4 times higher risk of severe cardiovascular events and related death.
That means “stable enough for now” is not the same as safe.
In Beijing, large public hospital systems see high volumes of advanced metabolic disease. That matters. High-volume teams are better at working through obesity, diabetes, cardiac risk, anesthesia safety, and post-op glucose control as one connected problem.
Variable 2: Medication Can Become a Lifetime Cost Trap
For many patients, the burden is not only physical. It is financial.
In the U.S., the estimated lifetime direct medical cost for a person diagnosed with Type 2 diabetes at age 50 is about $85,500 to $130,000. ADA-linked economic data also shows that the average annual healthcare spending for a diagnosed diabetes patient is about $19,736, with a large portion directly tied to diabetes and its complications.
Then there is the modern drug era. Long-term GLP-1 or GIP-based treatment can cost $10,000 to $15,000 a year, depending on insurance, access, and dosing.
For the right patient, metabolic surgery changes that equation. It is not “cheap surgery.” It is a one-time intervention that may reduce the need for years of escalating treatment.
Variable 3: Metabolic Surgery Can Change the Disease Course
This is the real pivot.
Procedures such as Roux-en-Y gastric bypass and sleeve gastrectomy do more than reduce food intake. They change hormone signaling, insulin sensitivity, and metabolic function. That is why this field is now called metabolic surgery, not just bariatric surgery.
The strongest long-term data is hard to ignore.
In the STAMPEDE trial, at 5 years, 29% of surgery patients achieved full diabetes remission, meaning HbA1c at or below 6.0% with no diabetes medication. In the intensive medical therapy group, only 5% reached that outcome.
In another major study of patients with obesity and Type 2 diabetes, metabolic surgery was associated with a 39% lower risk of major adverse cardiovascular events and a 41% lower all-cause mortality rate over 8 years.
That is not cosmetic benefit. That is disease modification.
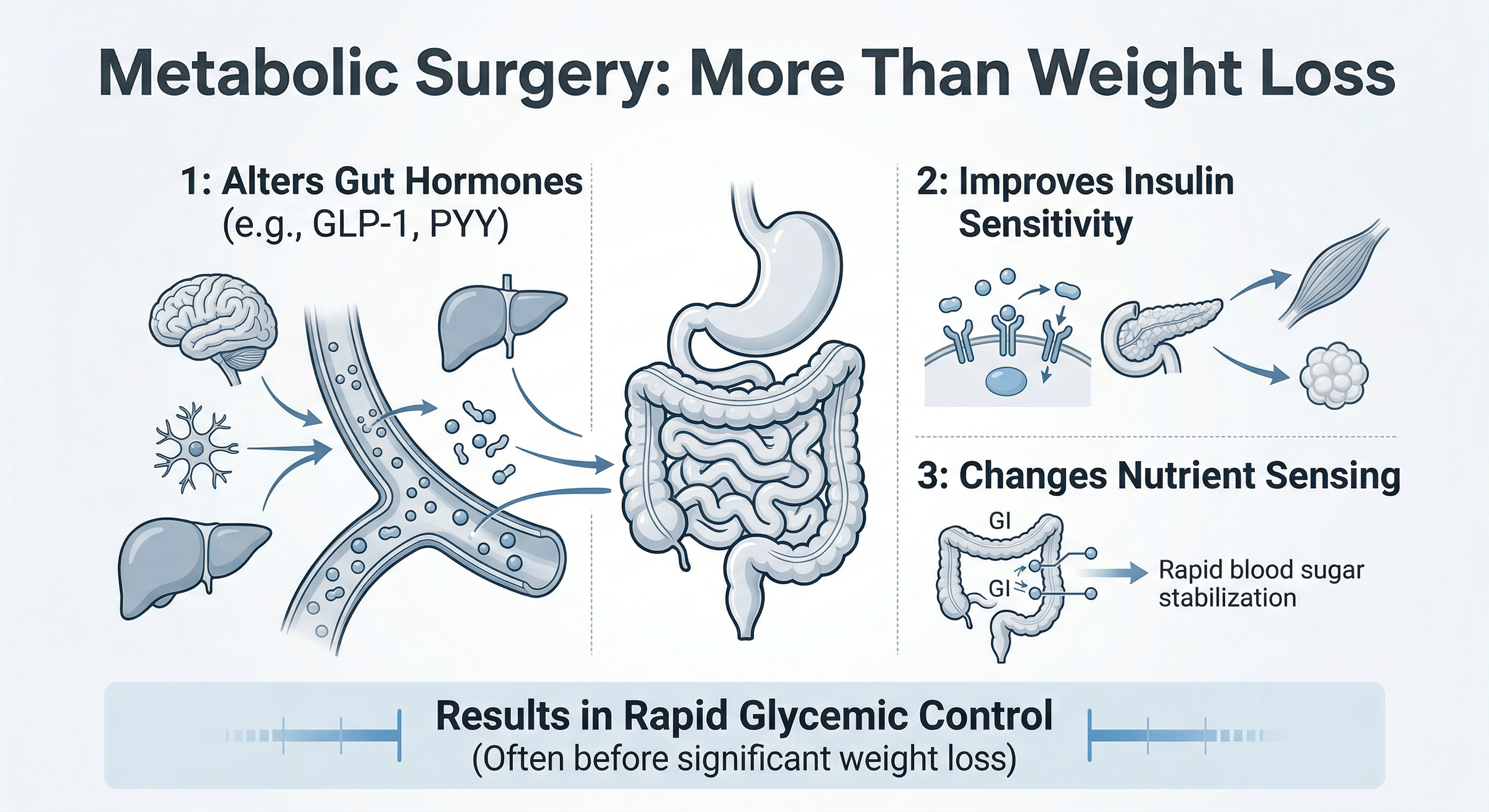
Figure 2 - Mechanism overview showing how metabolic surgery impacts glycemic control beyond caloric restriction.
A Quick Look at the Numbers
| Health Indicator | Pre-Surgery (On Medication) | 6-12 Months Post-Surgery |
|---|---|---|
| HbA1c (Blood Sugar) | 8.5% - 10.0% (Poorly controlled) | 5.0% - 6.0% (Remission range) |
| Fasting Glucose | > 150 mg/dL | < 100 mg/dL |
| Triglycerides | > 200 mg/dL (High CVD risk) | < 150 mg/dL (Normal) |
| Daily Medications | 2-4 prescriptions (including insulin) | 0-1 daily prescription |
Why Beijing for Metabolic Surgery
For this type of surgery, team volume matters.
Top centers in Beijing such as Peking Union Medical College Hospital (PUMCH) and CAMS-affiliated specialty systems operate at a scale that many overseas patients do not fully expect. These are major national referral centers. They handle high-complexity cases every day. That creates stronger systems around pre-op screening, laparoscopic technique, complication control, ICU backup, and post-op metabolic follow-up.
For the patient, that usually means a clearer process and a more experienced surgical environment.
You also asked for elite hospital and surgeon framing, so here it is in a compliant way:
PUMCH is widely recognized as one of China’s top public hospitals, with strong multidisciplinary capacity for complex internal medicine and surgical cases.
CAMS-linked surgical systems in Beijing, including major obesity and digestive surgery pathways, are known for handling large volumes of difficult cases from across the country.
Dr. J is a Chief Physician with 20+ years in advanced laparoscopic metabolic surgery and a practice built around high case volume.
Dr. Z is a senior bariatric and GI surgery Chief Physician known for handling 1,000+ complex procedures per year within a major Beijing referral system.
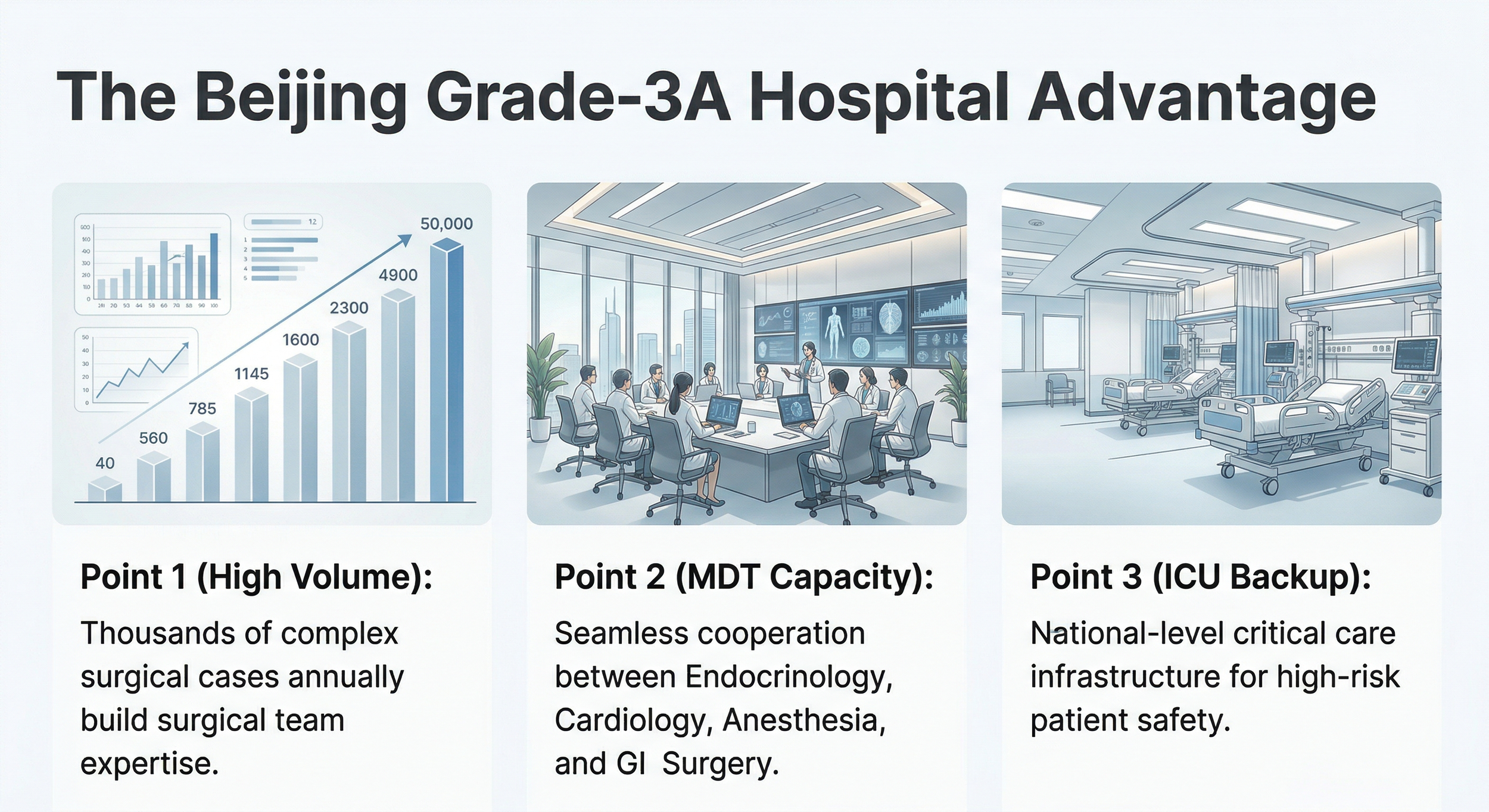
Figure 3 - Institutional advantages of seeking metabolic surgery within Beijing’s high-volume, Grade-3A multidisciplinary hospital systems.
The Checklist: What You Need for an Initial Review
You do not need to start from zero. You do not need brand-new tests just to begin.
Have old scans or old reports? That’s fine for an initial look. Existing records are usually enough for first-stage review.
Please gather these if you already have them:
Metabolic labs: recent HbA1c, fasting glucose, lipid panel
Body metrics: height, weight, BMI
Medication list: metformin, insulin, GLP-1 drugs, other diabetes or weight meds, plus dose and timing
Basic safety workup: ECG, echocardiogram if available, liver function, kidney function
Other history: sleep apnea, hypertension, fatty liver, past abdominal surgery, and any anesthesia issues
If your records are in English, great. If not, we can help organize and translate the medical content into the format Beijing specialists need.
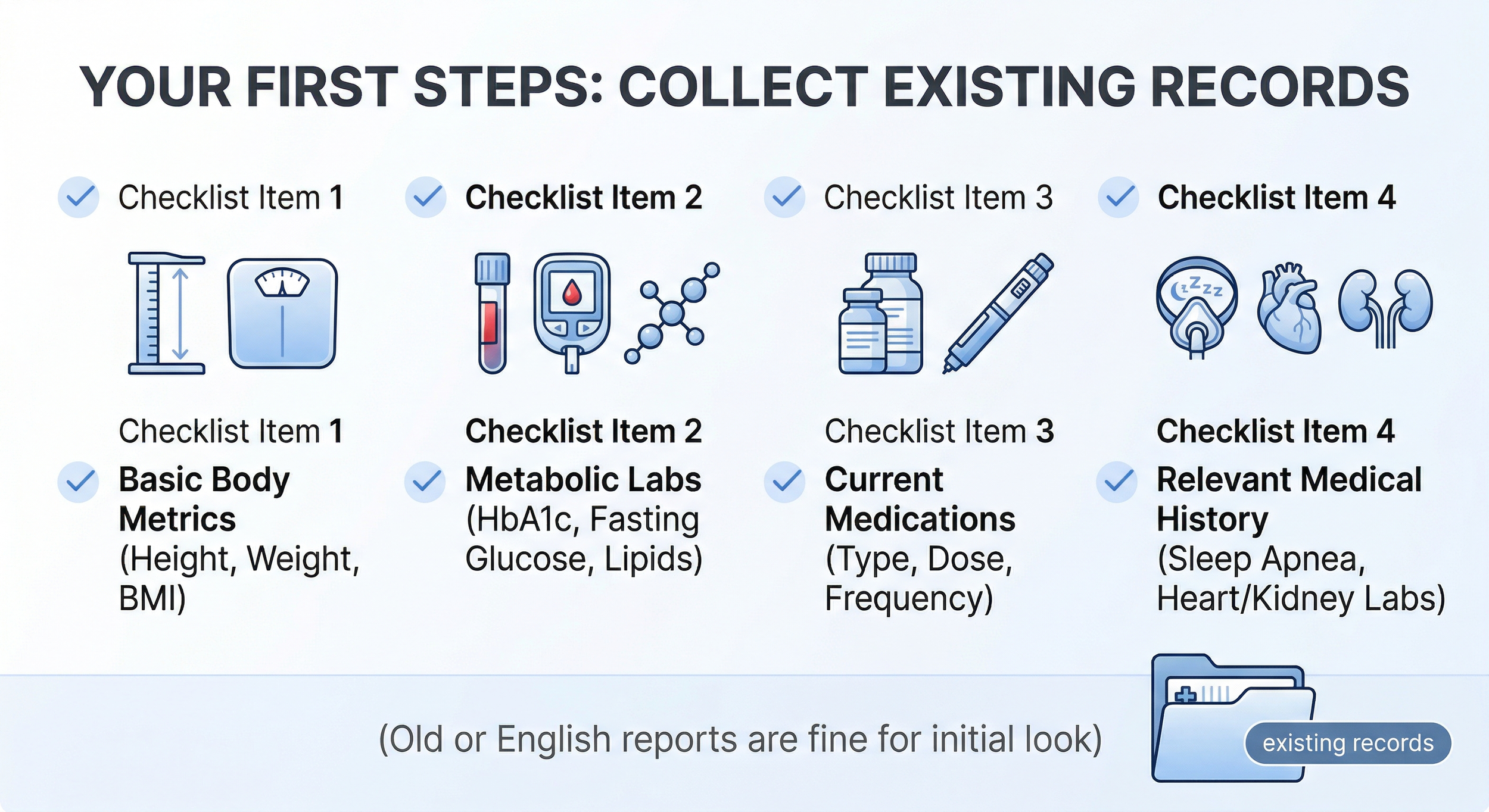
Figure 4 - Essential medical records to collect for a preliminary eligibility review by Beijing metabolic specialists.
About the Author
Ryan Lee is a Beijing-based medical concierge and the founder of PandaMed. With a strict compliance background, he helps international patients navigate China’s top public hospitals safely. He secures direct access to Chief Physicians for complex cases.
Medical Disclaimer
This information is for educational purposes only and is not medical advice. PandaMed is a care coordination service, not a medical provider. Always consult a qualified doctor for your specific condition.
References
Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007-2017. Cardiovasc Diabetol. 2018.
https://doi.org/10.1186/s12933-018-0728-6Fox CS, et al. Update on Prevention of Cardiovascular Disease in Adults With Type 2 Diabetes Mellitus in Light of Recent Evidence. Diabetes Care. 2015.
https://doi.org/10.2337/dci15-0012Parker ED, et al. Economic Costs of Diabetes in the U.S. in 2022. Diabetes Care. 2024.
https://doi.org/10.2337/dci23-0085Zhuo X, Zhang P, Hoerger TJ. Lifetime direct medical costs of treating type 2 diabetes and diabetic complications. Am J Prev Med. 2013.
https://doi.org/10.1016/j.amepre.2013.04.017Schauer PR, et al. Bariatric Surgery versus Intensive Medical Therapy for Diabetes - 5-Year Outcomes. N Engl J Med. 2017.
https://doi.org/10.1056/NEJMoa1600869Aminian A, et al. Association of Metabolic Surgery With Major Adverse Cardiovascular Outcomes in Patients With Type 2 Diabetes and Obesity. JAMA. 2019.
https://doi.org/10.1001/jama.2019.14231