
What Medical Records to Bring to China for Treatment
Travel plans are only one part of preparing for treatment abroad. For many international patients, the bigger worry starts right before departure: Will the doctors in China understand my case? What if I arrive missing something important?
That concern is valid. But the answer is usually not to bring every document you have ever received.
When patients prepare medical records for treatment in China, one of the most common mistakes is assuming that more paperwork is always better. In reality, top specialists need something more useful than volume. They need a clear, well-organized, clinically relevant record set that tells the story of your condition quickly and accurately.
If your materials are scattered across portals, mixed across languages, or buried in long hospital printouts, that can slow down review. For international patients coming to Beijing or other major Chinese hospitals, the goal is not to bring everything. The goal is to bring the right records, in the right format, in a clear order.
What Chinese Doctors Usually Need First
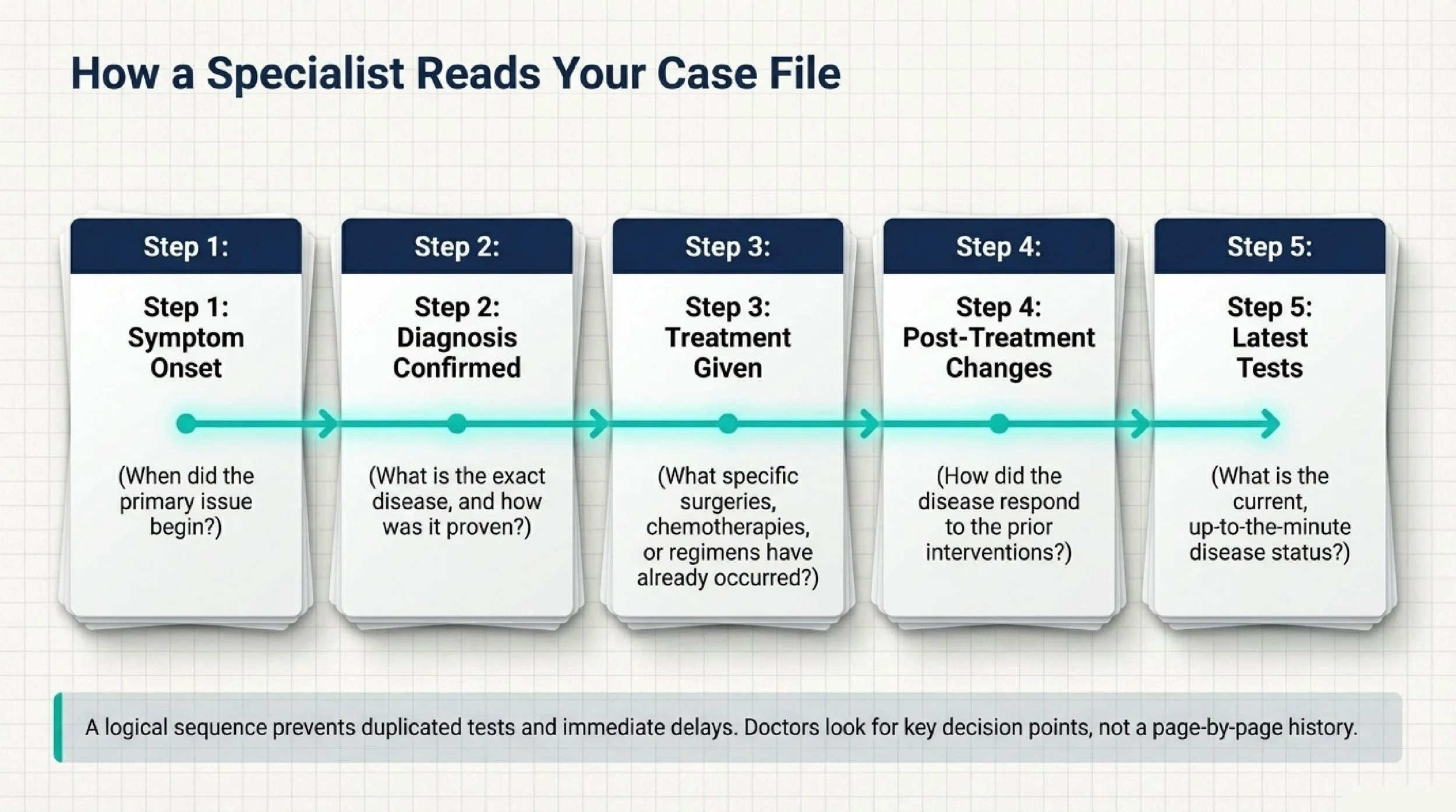
At the first specialist review, doctors are usually trying to answer a few practical questions very quickly. What is the diagnosis? How was it confirmed? What treatment has already been done? What happened after that? And what does the most recent imaging or pathology show now?
That means the most valuable records are usually the ones that define the diagnosis, show the treatment history, and clarify the current disease status.
The essential record types
| Document Type | What to Include | Why It Matters |
|---|---|---|
| Medical summary and timeline | A 1–2 page summary of symptom onset, diagnosis date, major treatments, key test results, and current status | This is often the fastest way for a specialist to understand the whole case |
| Pathology reports | Biopsy results, immunohistochemistry, molecular or genetic testing, and final diagnostic reports | These confirm the diagnosis and may affect whether repeat biopsy is needed |
| Imaging reports and raw files | Recent CT, MRI, PET-CT reports plus original DICOM files on disc or USB | Written reports help, but specialists often want the original images for review and planning |
| Surgical and treatment records | Operative notes, chemotherapy regimens, radiation details, discharge summaries, and procedure records | These show what has already been done and help avoid duplicated or conflicting treatment |
| Medication and allergy list | Current medications, generic names, doses, supplements, and known allergies | This is important for immediate safety and treatment planning |
Why Organization Matters More Than Volume
A specialist does not need 300 pages of loosely related printouts to understand a case. What helps most is a logical sequence.
In most cases, your file should tell a simple story in order:
when symptoms started → how the diagnosis was confirmed → what treatment was given → what changed afterward → what the latest tests show
That structure matters because first reviews are usually time-sensitive. The doctor is not trying to read every page of your history in detail at the start. They are trying to identify the key decision points quickly.
If the important pathology result is buried between routine nursing notes, or the most recent PET-CT is mixed with years-old lab slips, the review becomes slower and less efficient. In some cases, disorganized records can lead to duplicated tests or delayed treatment planning simply because the team cannot verify what has already been done.
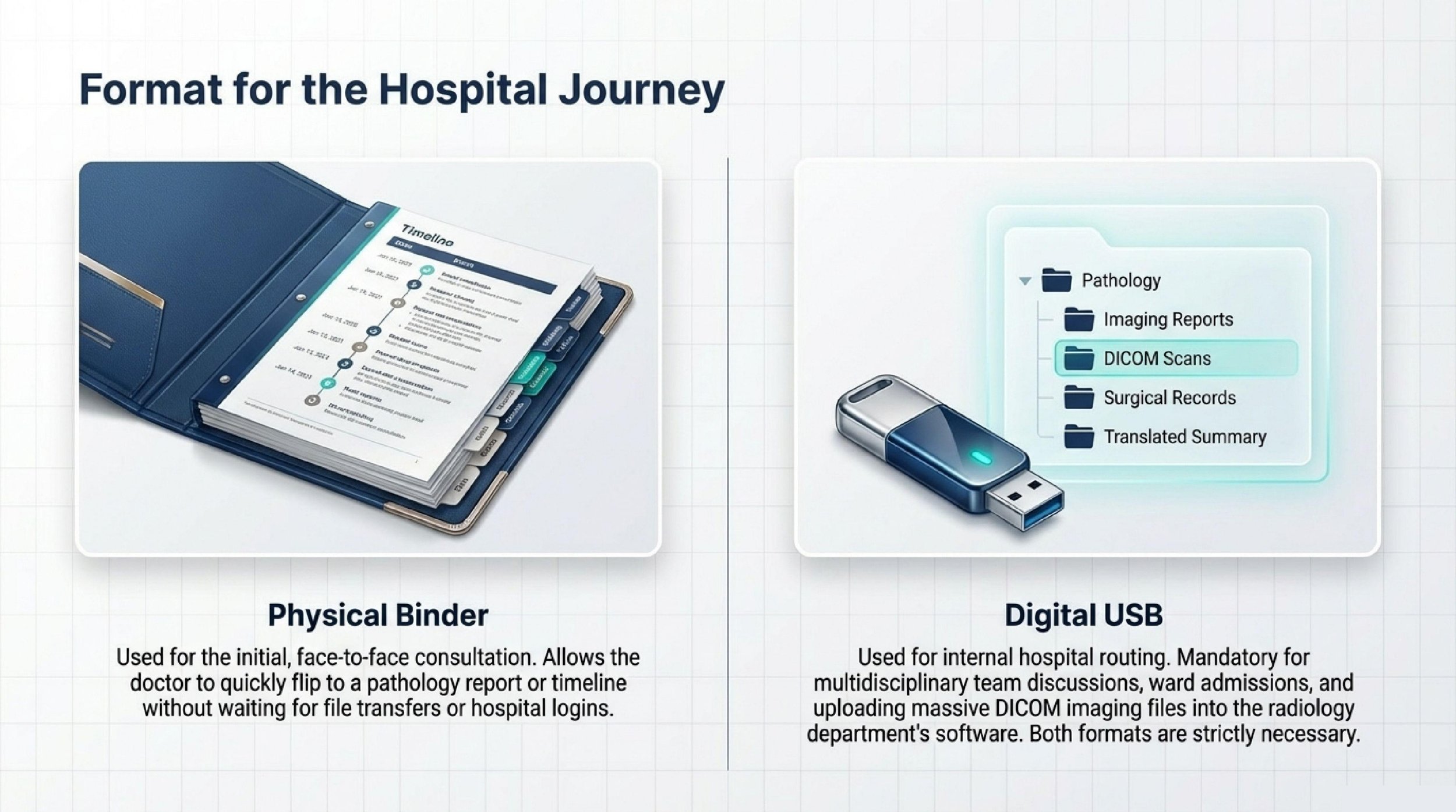
Bring Both Physical and Digital Copies
International patients should prepare both paper and digital records before traveling to China.
A physical binder is still useful during the first in-person consultation. It allows a doctor to quickly flip to the pathology report, treatment timeline, or imaging conclusion without waiting for a file transfer or login. For many patients, this remains the fastest way to support a face-to-face discussion.
Digital copies matter just as much. Once a hospital begins formal review, records often need to be shared internally for imaging review, multidisciplinary discussion, ward admission, or treatment planning. Having your records organized on a USB drive can make that process much smoother.
If possible, keep your digital files sorted into folders such as:
pathology
imaging reports
DICOM scans
surgical records
discharge summaries
blood tests
medication list
translated summary
This kind of structure makes a real difference when records need to be handed from one department to another.
Why You Need Both a Summary and the Original Data
Many patients ask whether a translated summary is enough. Usually, it is not enough by itself.
A short medical summary is extremely helpful because it gives doctors a fast overview of the case. It helps the nurse, resident, coordinator, and specialist understand the big picture right away. In many situations, this is the most efficient first document to translate.
But the original records are still the evidence behind that summary.
For example, a summary may say that a biopsy confirmed a specific diagnosis or that a scan showed progression after treatment. The specialist will still want to see the original pathology report or raw imaging to confirm those details. In other words, the summary creates speed, but the original files provide clinical proof.
That is why the best preparation usually includes both:
a clean, readable summary for fast understanding and the original reports and scan files for verification
The Records That Are Often Less Important
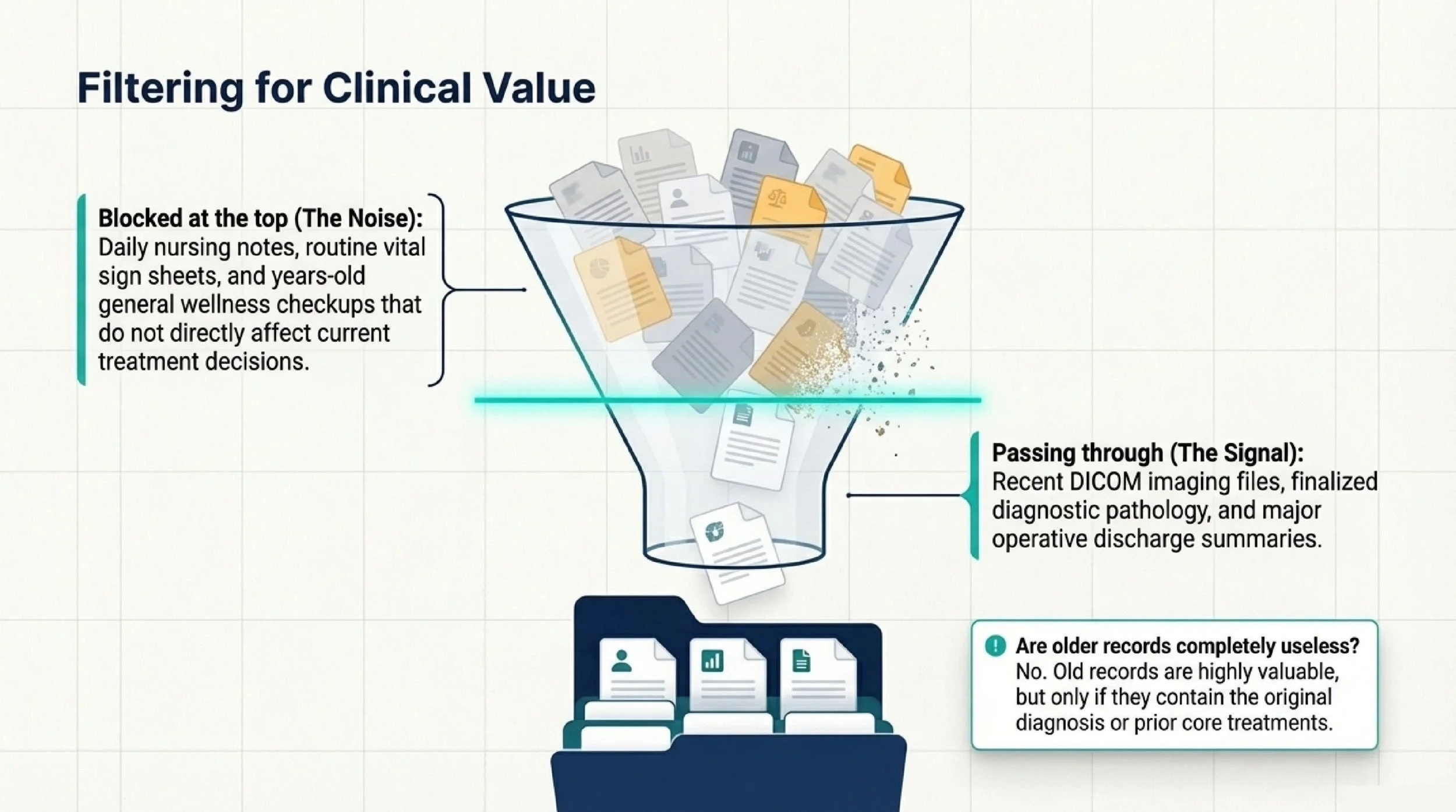
Patients often over-pack routine documents and under-pack the records that actually affect decisions.
In many cases, you do not need to print every daily nursing note, every routine vital sign sheet, or every general check-up from many years ago. These can add noise without adding much value, especially if they are not directly related to the current diagnosis or treatment decision.
That does not mean older records are useless. In fact, old records are often enough for an initial records check, especially if they include the original diagnosis, key pathology, prior treatment details, and recent imaging. But they should be selected carefully.
The goal is not to bring the largest stack. The goal is to bring the records that answer the main clinical questions.
Common Problems Caused by Disorganized Records
When materials are scattered, mixed-language, or incomplete, the most common result is not usually refusal. It is delay.
A doctor may decide to repeat recent bloodwork because the original results are hard to identify or verify. A radiologist may ask for another scan because only the written report is available but not the raw DICOM files. A treatment decision may be postponed because the pathology wording is unclear or the timeline of prior treatment is incomplete.
For international patients, these delays can affect much more than convenience. They can affect hotel stays, travel planning, family support arrangements, and the timing of the next medical step.
That is why record preparation is not just administrative. It is part of treatment readiness.
If Your Records Are Scattered, Start With What You Already Have
Many patients do not have a perfect file set when they first reach out. That is normal.
Some records may be spread across hospital portals. Some may exist only as screenshots, discharge packets, or CDs from different departments. Some may be in different languages. That does not mean the case cannot be reviewed.
In many situations, the best first step is simply to gather the materials you already have and identify the core records. If the file is scattered or difficult to organize, PandaMed can help structure the medically relevant parts of the case, prepare a clear timeline, and support translation of the documents most useful for a Beijing specialist review.
If you are unsure whether your existing records are enough, or which documents should be prioritized first, you can email what you already have to contact@pandamedglobal.com. Old records are often enough for an initial records check.
FAQ
Do I need to translate every page of my medical records?
No. In most cases, translating every routine page is unnecessary. The priority is usually the medical summary, pathology reports, imaging conclusions, operative notes, and major discharge summaries.
What if my hospital will not provide the raw imaging files?
In many countries, patients can request access to their imaging data through the hospital’s medical records or radiology department. If you are seeking treatment abroad or a second opinion, ask specifically for the original DICOM files on disc or USB if available.
Should I bring physical pathology slides or paraffin blocks?
In some complex cancer cases, the receiving hospital may want to review pathology again or run additional testing. If your local hospital allows release of pathology slides or paraffin blocks, it can be helpful to ask whether they should be carried or sent later if requested.
How recent should my records be?
It depends on the condition. For fast-changing diseases such as cancer, recent imaging and blood tests are often more useful if they are within the past 4 to 6 weeks. If your latest scans are older, be prepared for the possibility that repeat testing may be recommended after arrival.
If your case file is mixed across portals, languages, and document types, PandaMed can help you organize the core records for specialist review, prepare a clear timeline, and identify what matters most before travel. For record-preparation guidance or to check whether your current materials are enough to start, email contact@pandamedglobal.com.