
Lumbar Disc Herniation Surgery: What to Consider After Conservative Treatment Stops Working
You have done the usual first steps. Medications, physical therapy, and maybe injections. But the leg pain is still there, and now the real question is whether more waiting is reasonable or whether it is time to look at surgery. For international patients trying to compare treatment pathways, Beijing’s top public spine centers are worth understanding because they combine high surgical volume, advanced minimally invasive techniques, and faster specialist access than many Western systems.
Quick Decision Snapshot
| Decision Point | Typical Western Pathway | Top Beijing Public Hospitals |
|---|---|---|
| First-line treatment | Physical therapy, medication, and injections before surgical referral in many cases | Similar conservative-first approach, but often with earlier specialist imaging review in high-volume centers |
| Specialist wait time | Can be prolonged depending on local referral and insurance pathways | Often faster access to spine specialists and surgical triage through coordinated public-hospital pathways |
| Out-of-pocket cost | Often substantially higher in private-pay settings | Often substantially less expensive than private-pay care in the US or UK |
If you already have MRI scans, reports, clinic notes, or prior treatment records, you can send them to contact@pandamedglobal.com to check whether your current records are enough for an initial review and what to prepare next. Old records are often enough for an initial records check.
When the 4-6 Week Threshold Starts to Matter
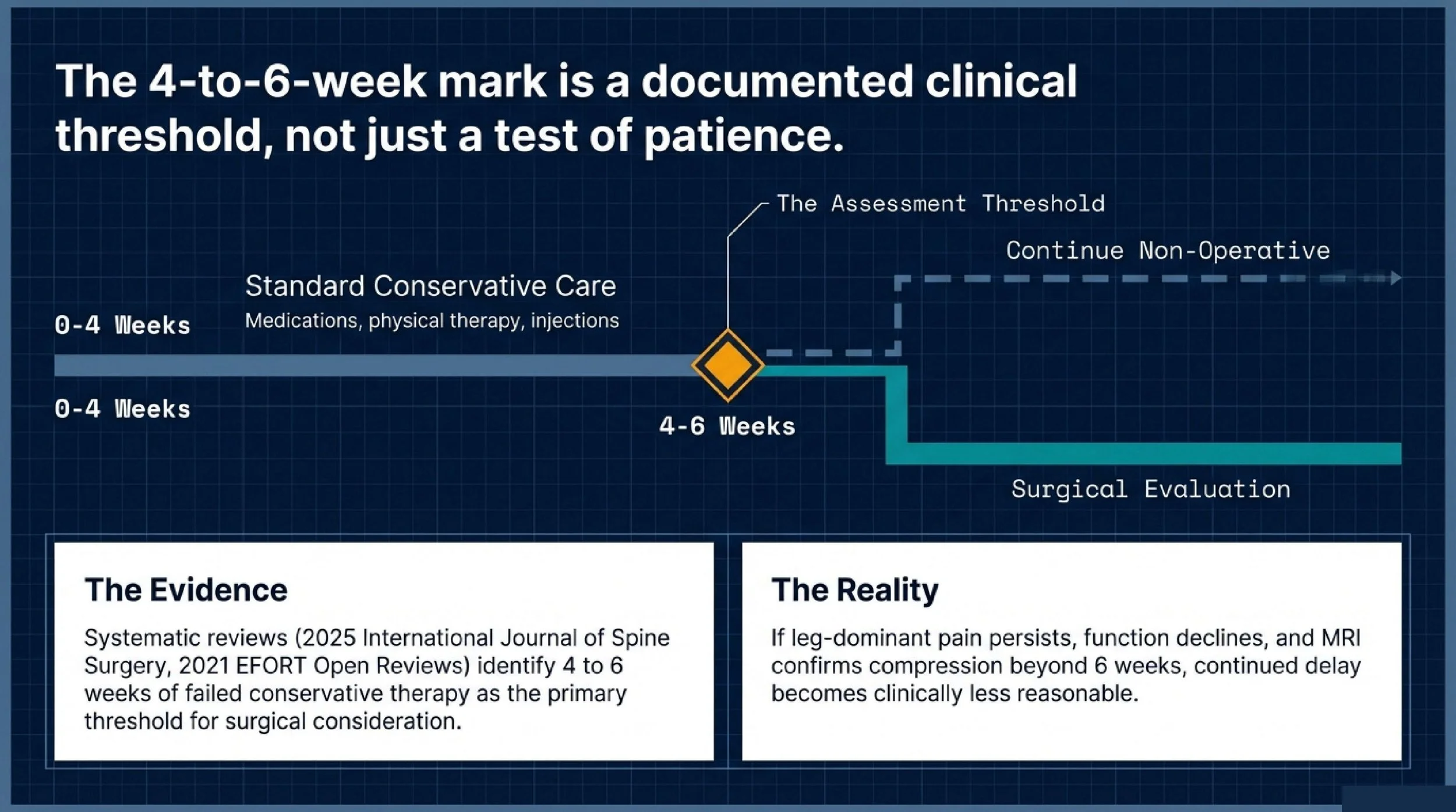
Most lumbar disc herniations should not go straight to surgery. That is why conservative treatment remains the standard starting point. But “keep waiting” is not an unlimited strategy, and the literature gives a clearer timeline than many patients expect.
A 2025 systematic review in the International Journal of Spine Surgery, covering 20 studies on lumbar disc herniation decision-making, found that failure of conservative treatment after 4 to 6 weeks was the most commonly cited threshold for moving toward surgical consideration. A 2021 review in EFORT Open Reviews similarly concluded that surgery becomes appropriate for lumbar disc herniation when patients fail to improve after six weeks of conservative care.
That does not mean everyone should have surgery exactly at week six. It means that when symptoms remain strong beyond that window, the decision should be reassessed using the full clinical picture: leg pain severity, neurologic findings, MRI anatomy, and functional decline.
In practical terms, if your pain is still radiating down the leg, you cannot sit or walk normally, and the MRI clearly shows a compressive disc herniation that matches your symptoms, continued delay becomes less reasonable.
Which Patients Are More Likely to Fail Conservative Treatment
Not all lumbar disc herniations behave the same way. Some improve with time and structured nonoperative care. Others are much less likely to settle down on their own.
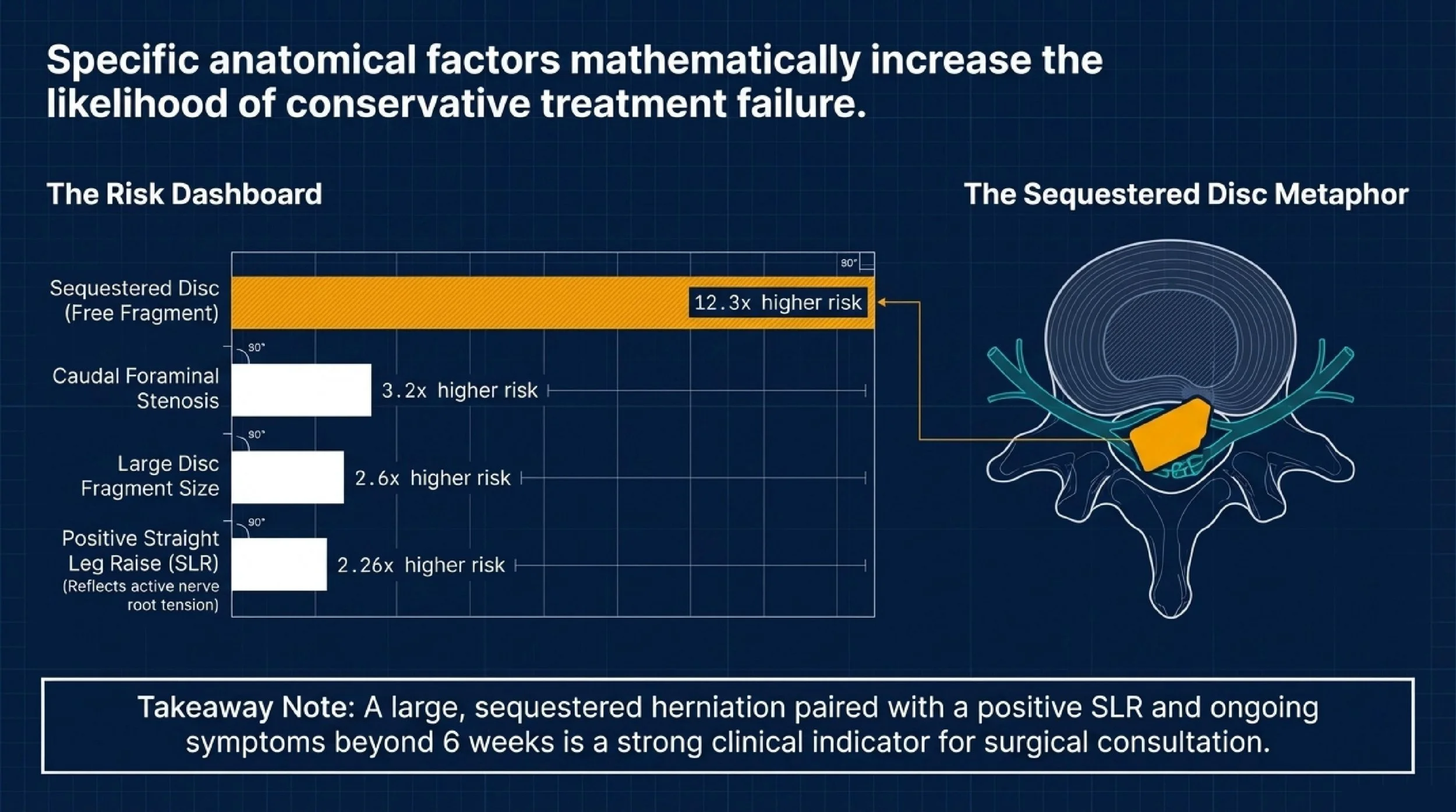
The source material identifies several predictors of conservative-treatment failure. A positive straight leg raising test carried an odds ratio of 2.26, suggesting that classic nerve root tension is a meaningful warning sign. Caudal foraminal stenosis had an odds ratio of 3.2, showing that coexisting narrowing around the exiting nerve makes nonoperative success less likely.
The strongest predictor listed was a sequestered disc herniation, with an odds ratio of 12.3. That matters because a free fragment is not just a bulge. It often reflects a more disruptive disc event and may correlate with persistent nerve compression. Large disc fragment size also predicted conservative failure, with an odds ratio of 2.6.
So the key pattern is not one isolated variable. It is the combination. If you have a large, sequestered herniation, a positive SLR, and symptoms persisting beyond 6 weeks, especially with progressive neurologic deficits, surgical consultation is warranted.
Your Surgical Options and the Trade-Off Behind Each One
Minimally Invasive Discectomy: Often the Best Fit for a Simple Nerve Compression Pattern
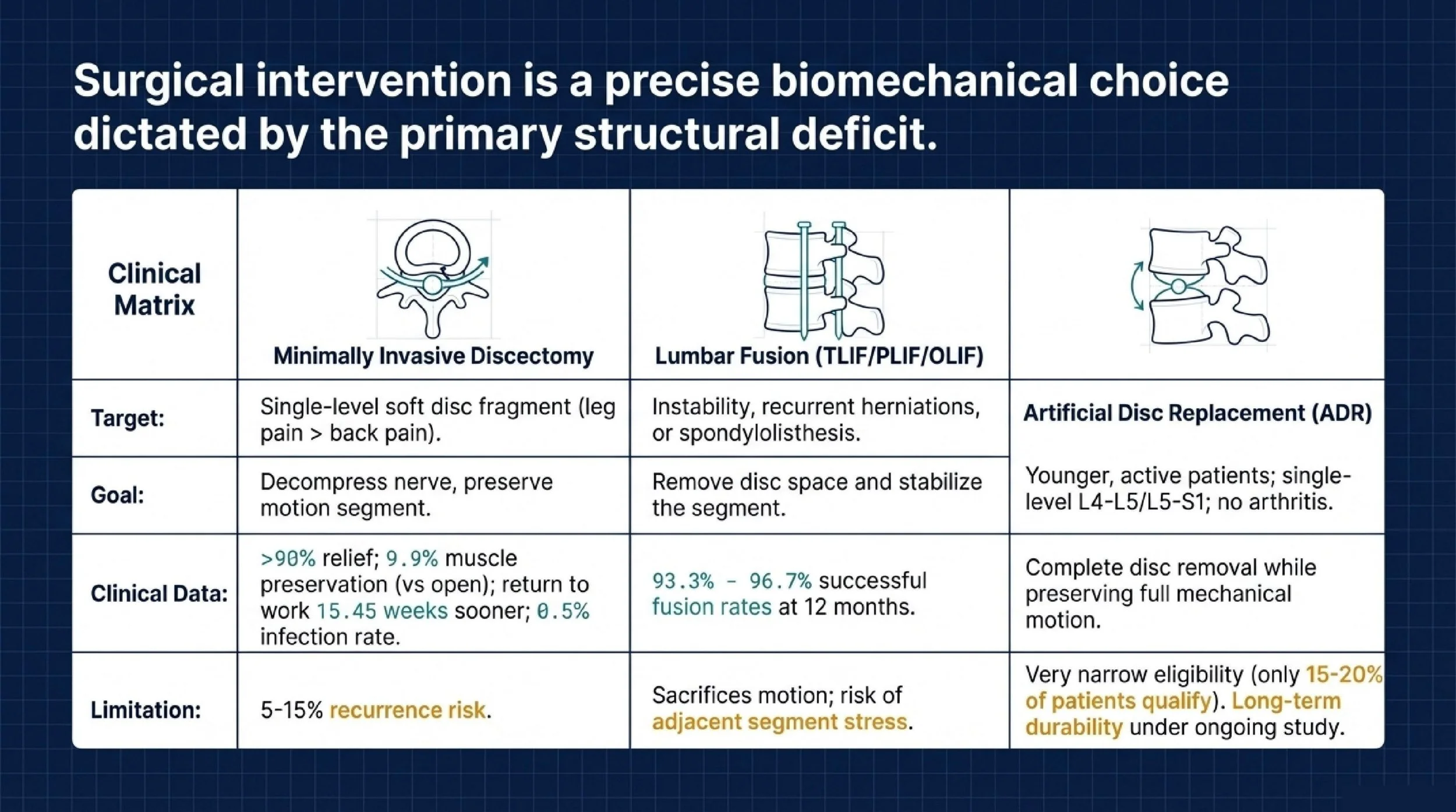
Microdiscectomy or endoscopic discectomy is usually the most direct operation when the problem is a single-level soft disc herniation, leg pain is more severe than back pain, and there is no significant spinal instability.
The idea is straightforward: remove the fragment that is compressing the nerve while preserving most of the disc and normal spinal motion. In well-selected patients, this remains the most common surgical solution for lumbar disc herniation.
The evidence cited in your source material is strong enough to make the practical advantages clear. Reported pain relief rates are greater than 90%. Paraspinal muscle cross-sectional area increased 9.9% compared with a 5.4% decrease in open surgery. Return to work was reported 15.45 weeks sooner than after open surgery, and infection risk was lower at 0.5% versus 1.6%.
Still, this is not a perfect operation. Recurrent herniation remains an issue, with 5% to 15% requiring reoperation for recurrence. Endoscopic approaches may also carry a higher risk of incomplete decompression in difficult anatomy. They are generally not ideal for calcified discs, severe stenosis, or instability.
Lumbar Fusion: More Relevant When the Disc Problem Comes With Instability
Fusion procedures such as TLIF, PLIF, or OLIF are not the standard answer for every lumbar disc herniation. They become more relevant when the disc herniation is part of a broader structural problem.
The most common situations are recurrent herniation at the same level, advanced disc degeneration with instability, or spondylolisthesis with herniation. In those settings, simply removing disc material may not solve the deeper mechanical issue.
Fusion removes the diseased disc, places a cage and bone graft, and stabilizes the segment with instrumentation. One major advantage is that it prevents reherniation at that same disc level because the disc space is no longer functioning as a mobile segment. The source material reports fusion rates of 93.3% to 96.7% at 12 months.
The trade-offs are also clear. Motion is sacrificed at the fused level. Recovery is longer. The operation is more invasive. And adjacent segments may take on higher stress over time, which is why adjacent segment disease remains part of the long-term discussion.
Artificial Disc Replacement: Motion Preservation, but Only for a Narrow Group
Artificial disc replacement, or ADR, sits in a different category. It removes the disc completely but replaces it with a prosthesis designed to preserve motion rather than eliminate it.
This approach is usually considered for single-level disc degeneration, typically at L4-L5 or L5-S1, in younger, active patients who want to maintain spinal motion and who do not have facet arthritis or instability.
Its appeal is obvious. It preserves motion, may reduce adjacent-segment stress compared with fusion, and recovery can be faster than fusion in properly selected patients.
But selection is strict. The source material estimates that only 15% to 20% of lumbar disc herniation patients qualify. It is generally contraindicated in osteoporosis, facet arthropathy, prior spinal surgery, and deformity. It also comes with higher implant-related cost and ongoing questions about durability beyond 10 to 20 years.
Why Beijing’s Top Spine Centers Matter for This Choice
Choosing the right surgery is only part of the decision. The other part is choosing a center that sees enough volume to recognize when a case is straightforward and when it is not.
That matters in lumbar disc herniation because many patients do not present with a “pure” disc problem. Some also have recurrent herniation, segmental instability, foraminal stenosis, calcification, or early deformity. In those cases, the wrong procedure can mean persistent symptoms, revision surgery, or avoidable recovery problems.
Beijing Jishuitan Hospital is one of China’s best-known orthopedic centers and is described in the source material as ranking No. 1 nationally in orthopedics. Its spine surgery department reports 3,300+ spine surgeries annually, 120,000+ outpatient visits, and 122 dedicated beds. The same source attributes to it more than 2,000 computer-assisted spine surgeries, along with leadership in navigation-assisted spine correction, percutaneous endoscopic discectomy, and the world’s first 5G telerobotic spine surgery. For patients exploring minimally invasive lumbar procedures, that depth of technical exposure matters.
Peking University People’s Hospital is also an important spine referral center in Beijing. According to the source material, it established one of China’s first specialized spine surgery wards in 2001. Its department reports 500+ complex spine surgeries annually, while one senior surgeon profile in the same source is associated with 700+ spine surgeries per year. The hospital is noted for complex cervical disease, spinal deformity correction, and minimally invasive techniques, which can be especially relevant when a lumbar case turns out to involve more than a routine discectomy.
Peking Union Medical College Hospital (PUMCH) remains one of China’s most recognized national referral institutions and is described in the source as consistently ranking among the country’s top five orthopedic centers. Its orthopedic department metrics include 5,000+ annual surgical cases, 150,000+ outpatient visits, 132 beds, and 262 advanced MISS procedures in 2021, including UBE, endoscopic fusion, and OLIF. For patients who need a broad multidisciplinary view rather than a one-procedure answer, PUMCH is especially relevant.
Where an anonymous surgeon profile is useful, the source material also supports one senior profile:
Dr. L is a senior spine specialist with annual volume reported at 700+ spine surgeries, with experience in complex spine disease, deformity correction, and minimally invasive techniques.
If your MRI report mentions more than a simple disc protrusion, or if you are unsure whether your symptoms match the imaging, you can email your current records to contact@pandamedglobal.com. Old records are often enough for an initial records check, and that is often the fastest way to understand what to prepare next.
What Patients Often Misunderstand About Surgery Timing
One common mistake is thinking conservative care means doing nothing. It does not. True conservative management is usually a structured trial of medication, physical therapy, activity modification, and sometimes injections, followed by reassessment.
Another mistake is assuming the MRI alone decides everything. It does not. Surgery becomes more relevant when imaging matches the pain pattern, exam findings, and level of disability.
The third mistake is waiting too long just because the pain is technically tolerable. Persistent radicular pain, worsening weakness, or a large sequestered fragment can all change the risk-benefit balance. The real question is not whether you can endure more time. It is whether more time is likely to change the outcome.
The Checklist
You do not need brand-new records before asking for an initial review. Existing records are often enough to start.
For lumbar disc herniation, the most useful materials are:
MRI or CT scans
DICOM files are preferred when available, ideally performed within the last 6 months.
Clinical notes from your treating physician
Especially notes documenting neurologic findings, pain distribution, straight leg raising test, and current diagnosis.
Conservative treatment history
Include medications, physical therapy, and injections, with dates and outcomes if possible.
Current symptom summary
Describe pain location, numbness, weakness, walking tolerance, sitting tolerance, and sleep disruption.
Previous surgical records
If you have had prior spine surgery, include operative notes, discharge summary, implant details, and follow-up imaging.
Family / Logistics
If you are traveling with family, or you want to understand visas, lodging, appointment flow, interpretation, or general Beijing care coordination, you can email contact@pandamedglobal.com. That can help you understand the practical steps before deciding whether a Beijing evaluation makes sense.
Author Bio
Ryan Lee is a Beijing-based medical concierge and the founder of PandaMed. With a strict compliance background, he helps international patients navigate China's top public hospitals safely. He secures direct access to Chief Physicians for complex cases.
Medical Disclaimer
This information is for educational purposes only and is not medical advice. PandaMed is a care coordination service, not a medical provider. Always consult a qualified doctor for your specific condition.
References
International Journal of Spine Surgery (2025). Indications for surgery versus conservative treatment in the management of lumbar disc herniations: A systematic review. PMID: 41078967.
EFORT Open Reviews (2021). Management of Lumbar Disc Herniation: A Systematic Review. PMID: 38034203.
Journal of the Medical Association of Thailand (2012). Factors predicting failure of conservative treatment in lumbar-disc herniation. PMID: 22994027.
Journal of Clinical Neuroscience (2007). Optimal duration of conservative treatment for lumbar disc herniation depending on the type of herniation. PMID: 17107804.
Global Spine Journal (2019). Endoscopic Versus Open Laminectomy for Lumbar Spinal Stenosis: An International, Multi-Institutional Analysis of Outcomes and Adverse Events. PMID: 32707015.
European Spine Journal (2022). Overweight and smoking promote recurrent lumbar disk herniation after discectomy. PMID: 35072795.
International Journal of Spine Surgery (2025). Outcomes Comparison Between Oblique Lumbar Interbody Fusion and Minimally Invasive Transforaminal Lumbar Interbody Fusion in Low-Grade Spondylolisthesis: A Randomized Clinical Trial. PMID: 41067932.