
Navigation-Assisted and 5G Remote Spine Surgery in Beijing for Complex Spine Conditions
SEO Title: Navigation-Assisted and 5G Remote Spine Surgery in Beijing: Precision Options for Complex Spinal Cases
If you have been told you may need spine surgery for scoliosis, spinal stenosis, fracture, or a failed prior fusion, the decision can feel heavy. The main question is not just whether surgery is needed. It is whether your case needs a higher level of precision, planning, and surgical experience. Beijing’s top public hospitals are among the centers international patients often look at when they want complex spine care in a high-volume setting.
Quick Decision Snapshot
| Care Question | US / UK Typical Pathway | Top Beijing Grade-3A Public Hospitals |
|---|---|---|
| First-line treatment after meds fail | Often months before specialist review and surgical planning | Faster multidisciplinary review, often with spine surgery input sooner |
| Specialist wait time | Commonly 3 to 8 months | Often around 2 to 3 weeks through coordinated access |
| Out-of-pocket cost | Often far higher in private-pay systems | Usually substantially lower than the US or UK private pathway for comparable complex surgery |
If you already have MRI scans, X-rays, CT, operative notes, or discharge records, you can send what you have now to contact@pandamedglobal.com. In many cases, old records are often enough for an initial records check, and you can find out what to prepare next without waiting for brand-new testing.
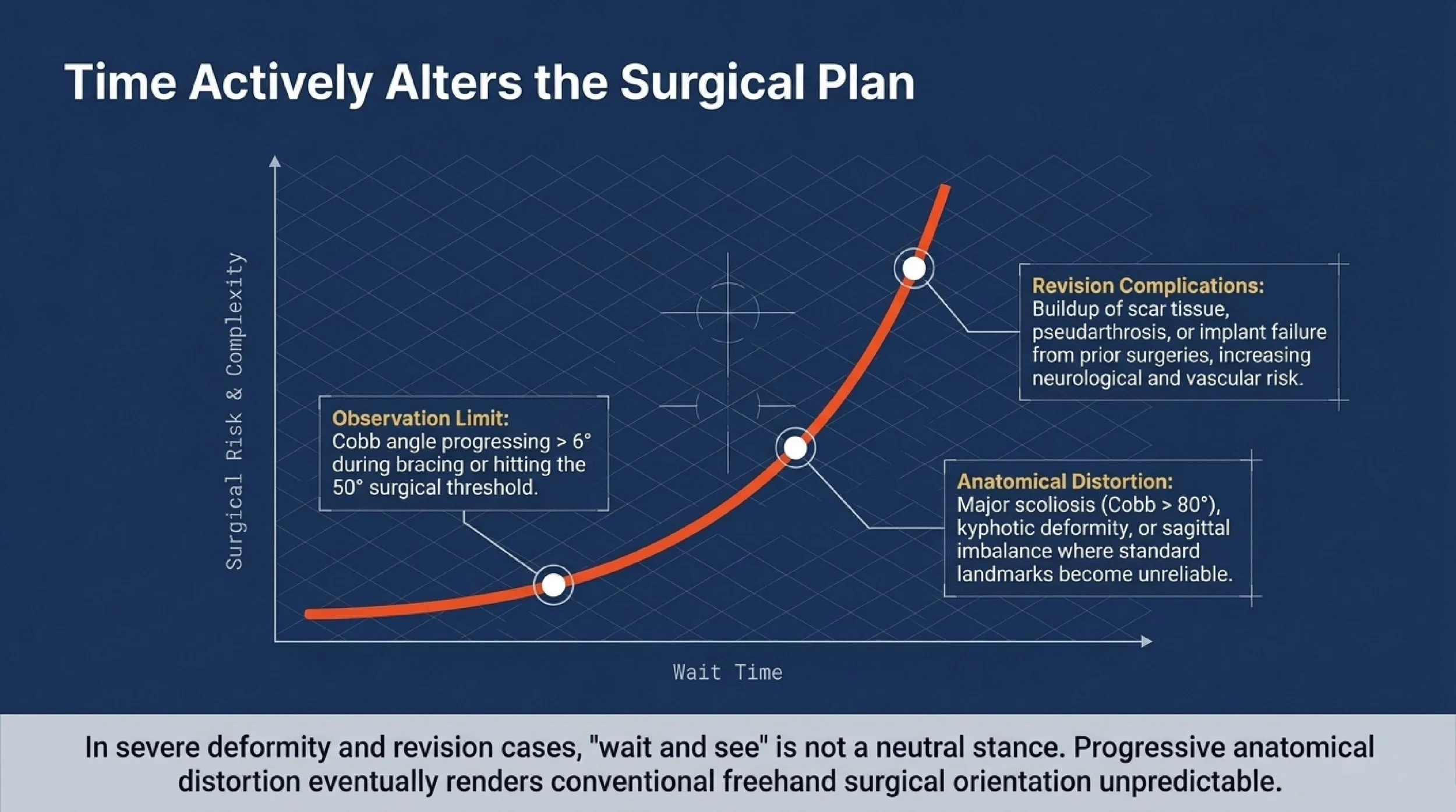
Why You Cannot Just "Wait and See"
For some spine problems, time changes the surgical plan. It can also change the technical difficulty and the risk profile.
When deformity progression stops being safe to watch
In scoliosis and other spinal deformities, observation has limits. If the Cobb angle keeps progressing by more than 6 degrees during bracing, or already reaches the common surgical threshold of 50 degrees, continued delay may allow the deformity to become harder to correct and more likely to affect alignment, pain, and long-term function.
This matters even more in severe deformity. In major scoliosis with Cobb angle above 80 degrees, kyphotic deformity, or sagittal imbalance, standard anatomical landmarks may no longer be reliable during surgery. Navigation-assisted systems can help the surgeon place pedicle screws more accurately in rotated, narrow, or dysplastic vertebrae, especially when multilevel osteotomy and fixation are required.
Why revision spine surgery is different from first-time surgery
Revision cases are not just “another spine operation.” They often involve scar tissue, prior implants, altered bone landmarks, pseudarthrosis, implant failure, or adjacent-segment disease. In these situations, conventional exposure and freehand orientation can become less predictable.
Navigation and robotic assistance may help reduce the risk of wrong screw trajectory in anatomy that has already been changed by prior fusion. That matters because revision cases can carry a higher risk of neurologic or vascular injury if the anatomy is distorted.
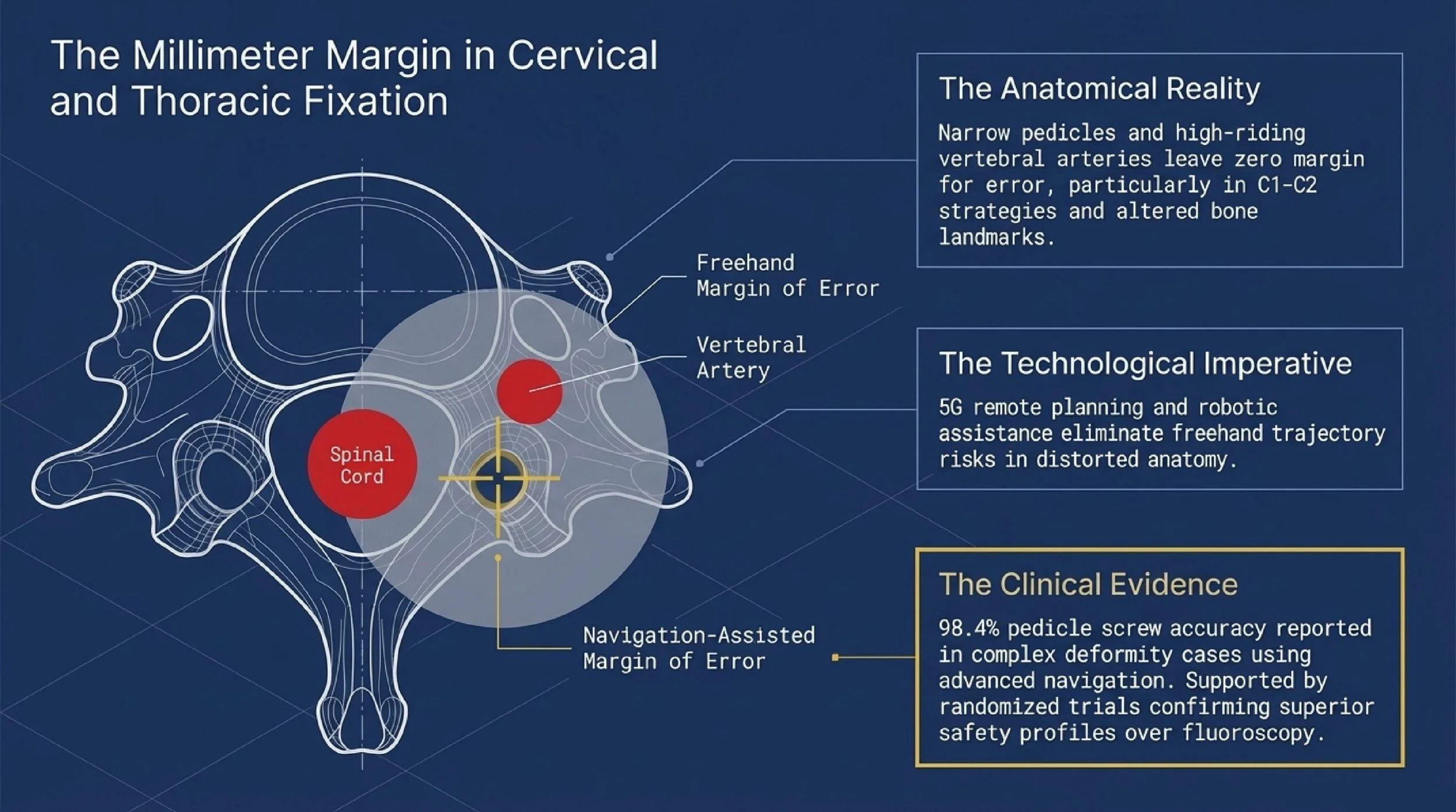
Why millimeters matter in cervical and upper thoracic surgery
The cervical spine and parts of the thoracic spine leave very little room for error. Narrow pedicles, vertebral artery variation, and proximity to the spinal cord all raise the stakes. In upper cervical fixation, including C1-C2 strategies, even a small deviation may have major consequences.
This is where image guidance and robotic planning become more important, especially in patients with congenital variation, high-riding vertebral artery anatomy, prior surgery, fracture, or severe degeneration.
Published evidence supports this direction. A randomized study in the thoracic spine reported better pedicle screw accuracy with computer-assisted navigation compared with conventional techniques. A prospective randomized trial in thoracolumbar surgery found robot-assisted screw insertion to be safe and accurate compared with fluoroscopy-assisted placement. A 2021 systematic review and meta-analysis in Journal of Neurosurgery: Spine also compared fluoroscopic and navigation-based techniques in cervical pedicle screw fixation and supported the value of navigation in high-risk anatomy.
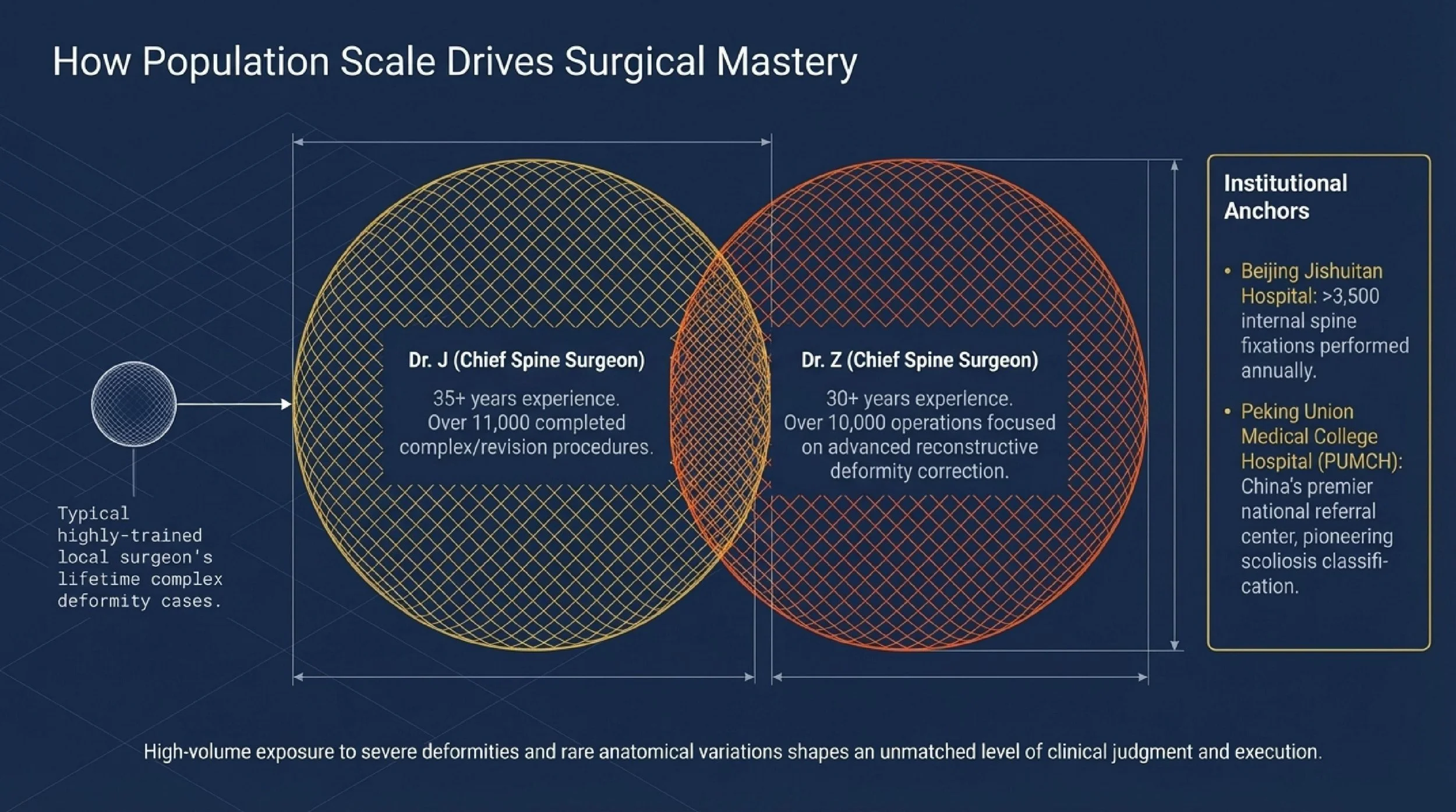
Why Beijing’s high-volume centers matter
Complex spine surgery is one of the clearest areas where case volume matters. High-volume centers tend to see more severe deformity, more revision surgery, more rare anatomical variation, and more technically difficult fixation cases. That repeated exposure shapes judgment, planning, and execution.
For international patients, two Beijing hospitals are especially relevant to this topic:
Beijing Jishuitan Hospital is widely recognized in China for complex orthopedic and spine surgery. Plain-text institutional attribution from the user’s draft notes that its spine service performs more than 3,500 internal fixation procedures per year and has reported pedicle screw accuracy of 98.4% in complex deformity cases using advanced navigation and robotic techniques.
Peking Union Medical College Hospital (PUMCH) is one of China’s best-known national referral centers. The user’s source notes its role in scoliosis classification research and its strength in congenital deformity, rare disease, and multidisciplinary case management.
For patients who need a surgeon profile rather than a public-facing doctor name, two representative senior profiles from the user’s material would look like this:
Dr. J is a chief spine surgeon with more than 35 years of experience and over 11,000 completed complex spine procedures, with particular focus on minimally invasive spine surgery and revision surgery.
Dr. Z is a chief spine surgeon with more than 30 years of experience and more than 10,000 complex spine operations, with long-term focus on deformity correction and advanced reconstructive spine surgery.
If your case is complex, or you are not sure whether your current MRI, CT, standing full-spine X-rays, or old operative records are enough, email what you already have to contact@pandamedglobal.com. Existing records are often enough to start, and you can get practical guidance on record preparation and next steps.
The Checklist
You do not need to wait for brand-new records before asking for an initial review. In many cases, existing records are often enough to start.
For a complex spine case, these are the most useful items:
Imaging Full-spine standing X-rays in anteroposterior and lateral views, CT with 3D reconstruction, and the most recent MRI. Original DICOM files are preferred, whether from CD export or cloud link.
Bone quality A DEXA bone density scan can be important in older adults, revision cases, and patients with suspected osteoporosis because bone quality may affect screw choice, fixation strategy, and whether cement augmentation is considered.
Past treatment and surgical records If this is a revision case, prior operative notes, implant details, fusion status, discharge summaries, and follow-up imaging are highly useful.
Neurologic status Any recent motor or sensory exam, clinic note describing weakness or numbness, and EMG testing if radiculopathy has been evaluated.
Current symptom timeline A simple summary helps: when pain started, whether walking distance has dropped, whether posture or balance is worsening, and whether bowel, bladder, or progressive neurologic symptoms are present.
Travel, Family, and Beijing Care Coordination
If you are planning to come with a spouse, parent, or child, or you need help understanding visas, lodging, appointment flow, medical translation, hospital navigation, or Beijing care coordination, you can email contact@pandamedglobal.com. The goal is not to replace medical advice. It is to help you understand the practical steps before and during care in Beijing’s public hospital system.
Author Bio
Ryan Lee is a Beijing-based medical concierge and the founder of PandaMed. With a strict compliance background, he helps international patients navigate China's top public hospitals safely. He secures direct access to Chief Physicians for complex cases.
Medical Disclaimer
This information is for educational purposes only and is not medical advice. PandaMed is a care coordination service, not a medical provider. Always consult a qualified doctor for your specific condition.
References
CLEAR Scoliosis Institute (2024/2025 Cost Analysis).
Chinese Journal of Traumatology (English Edition). 2010. Pedicle screw placement in the thoracic spine: a randomized comparison study of computer-assisted navigation and conventional techniques.
Journal of Neurosurgery: Spine. 2019. Safety and accuracy of robot-assisted versus fluoroscopy-assisted pedicle screw insertion in thoracolumbar spinal surgery: a prospective randomized controlled trial.
Journal of Neurosurgery: Spine. 2021. The comparative accuracy and safety of fluoroscopic and navigation-based techniques in cervical pedicle screw fixation: systematic review and meta-analysis.
Scientific Reports. 2025. Modified classification system of high-riding vertebral artery for the C2 screw placement strategy: a large-scale, cross-sectional study.
Professor Li – Expert’s Personal Social Media Profile. Plain-text attribution only.