
Pituitary Adenoma Medication Intolerance: Endoscopic Surgery and MDT Pathways in Beijing
SEO Title: Pituitary Adenoma Medication Intolerance: Surgical Options and Timelines in Beijing
You started with the standard path. For many pituitary adenomas, that means dopamine agonists like cabergoline or bromocriptine first.
But sometimes that path breaks down fast. The side effects are too much. Or the tumor does not respond the way it should. When that happens, the next step should not be guesswork. In Beijing, high-volume pituitary teams can review imaging, hormone labs, visual risk, and surgical timing in one coordinated path.
TL;DR: What usually happens next?
| Key Issue | Typical first-step approach in many Western settings | What high-volume Beijing centers may offer |
|---|---|---|
| First-line treatment | Medication first, then later surgical review if side effects or resistance become a problem | Earlier parallel review by endocrinology, neurosurgery, radiology, and sometimes radiotherapy when the medication path is failing |
| Specialist wait time | Can involve staggered appointments across separate departments | Top public hospital teams may evaluate the case through an MDT-style route with faster internal coordination once records are organized |
| Out-of-pocket cost | Often depends on private access, insurance limits, imaging duplication, and repeat consultations | Costs vary by case, but public-hospital pathways in Beijing are often explored by patients seeking senior specialist access with strong surgical volume |
Have old MRI scans, lab reports, discharge notes, or medication records already? That is often enough for an initial records check. You can email your current materials to contact@pandamedglobal.com to ask whether the file set is workable and what to prepare next. You do not need to wait for brand-new imaging before asking about next-step coordination.
Figure 1 - Visual summary comparing the challenges of medication intolerance to the potential advantages of high-volume care pathways in Beijing.
Why You Cannot Just “Wait and See”
If the drug is causing severe side effects, many patients try to stop and hope things settle down. That can be risky. The real question is not just whether the medication is unpleasant. The real question is whether the tumor can safely stay on a medication-first path at all.
1) Tumor size and pressure on the optic pathway
This is one of the first things that matters.
If a pituitary macroadenoma is growing upward and pressing on the optic chiasm, the situation changes. At that point, the issue is no longer just hormone control. It becomes a space problem inside the skull. Vision loss can become the main risk.
That is why old MRI scans still matter. A specialist team can often tell a lot from prior imaging, even before a new scan is arranged. In Beijing, large pituitary and skull base teams handle high numbers of endoscopic transsphenoidal cases. High volume usually means better pattern recognition, better control in tight anatomy, and smoother decompression planning when vision risk is on the table.
At Peking Union Medical College Hospital (PUMCH), pituitary care is not isolated inside one department. Publicly available institutional information shows a mature pituitary pathway involving endocrinology, neurosurgery, radiology, and radiotherapy coordination. For international patients, that matters because the decision is often not “medicine or surgery” in the abstract. It is whether the case still belongs on a medical path once the visual and anatomical risk is reviewed.
2) Medication intolerance is not just “bad side effects”
For prolactinomas and some other functional pituitary adenomas, dopamine agonists are standard first-line treatment. But intolerance is real. Severe nausea, dizziness, orthostatic symptoms, or major mood changes can make long-term use impossible.
Once that happens, the question becomes more technical:
Is the patient truly intolerant at clinically meaningful doses?
Has the tumor shown resistance?
Is the drug still worth pushing?
Or is surgery now the safer second-line path?
This decision should not be made in a vacuum. It needs hormone data, medication history, MRI anatomy, and symptom burden looked at together. In high-volume Beijing centers, that combined review is one of the biggest advantages. The team is used to cases where the standard script no longer fits.
3) MDT planning changes the quality of the decision
A pituitary case can look simple from one angle and risky from another.
An endocrinologist may focus on hormone control. A neurosurgeon may focus on the surgical corridor and tumor invasion. A radiologist may see details in the cavernous sinus or optic apparatus that change the whole risk picture. If those views stay separated, patients lose time.
That is why multidisciplinary review matters so much in medication-intolerant cases. At top Beijing institutions, coordinated pituitary pathways reduce the usual loop of separate referrals. Instead of asking one doctor at a time, the case can be framed around one key question: Is there still a safe medical path, or is it time to move toward surgery and perioperative hormone planning?
If your case feels stuck between those two paths, you can send your current MRI reports, image files, hormone labs, and medication history to contact@pandamedglobal.com and ask what records usually matter first. Even older records are often enough to start organizing the file and clarifying the next communication step.
Figure 2 - Diagram illustrating the crucial medical comparison between a focus on hormonal control versus the potential need for surgical decompression when a pituitary macroadenoma threatens vision.
Why Beijing gets attention for pituitary surgery
If surgery becomes part of the discussion, experience matters. A lot.
The main operation here is usually endoscopic transsphenoidal surgery, which reaches the pituitary through the nasal corridor. It is minimally invasive in concept, but not simple in execution. The anatomy is tight. The margin for error is small. And some tumors are invasive, fibrous, or wrapped around structures that make the plan much harder than the MRI report suggests.
This is where Beijing stands out.
PUMCH has reported very high dedicated pituitary surgery volume and a formal pituitary joint-clinic model. That means patients are not bounced between disconnected departments. The hospital is one of the most recognized top-tier public hospitals in China, especially for complex endocrine and surgical coordination.
Beijing Tiantan Hospital is one of the biggest neurosurgical centers in China. Its surgical scale is massive. Publicly described volume data show an extremely high annual neurosurgical load, including a large number of minimally invasive endoscopic procedures in the skull base and pituitary region. For patients who may need surgery after medication failure, that kind of repetition matters.
High volume does not guarantee a specific outcome. But in pituitary and skull base work, it usually means sharper execution, better internal teamwork, and more mature complication management.
Figure 3 - Diagram demonstrating the multi-specialist approach of high-volume Beijing pituitary pathways, showcasing the MDT decision-making flow.
Specialist profiles
Your case in Beijing is not just about the hospital name. It is about who actually reviews it.
Dr. H is a Chief Physician in Neurosurgery at a top Beijing brain center. He has more than 20 years of experience in pituitary and skull base surgery and works inside a service line that handles very high annual volumes of endoscopic and complex tumor surgery. He also trained internationally in the United States.
Dr. E is a Chief Physician in Endocrinology at a major Beijing endocrine center. He focuses on pituitary disease, hormone staging, medication-pathway failure, and long-term endocrine planning. For patients who cannot stay on standard dopamine agonists, that endocrine judgment is just as important as the surgery itself.
When the standard path stops working
A useful way to think about Beijing’s advantage is this: the best centers do not just repeat the first failed plan. They rebuild the pathway.
Public case reporting from major Beijing institutions has described severe pituitary tumor cases with visual compression and invasive growth that required staged management. In those kinds of cases, surgery was used to relieve pressure and re-open the treatment path, while endocrine management was used to stabilize the long-term picture after that.
That does not mean every medication-intolerant prolactinoma needs surgery. It means the next step should be based on structure, not hope. If the patient cannot tolerate the drug, if the tumor is large, or if vision is at risk, the decision should move fast and be made by the right team.
What records do you need?
You do not need to gather everything perfectly before asking for help. Start with what you already have.
The basic records checklist
MRI report
MRI image files if available, ideally DICOM files from a CD or download link
Pituitary hormone labs
Medication history, including exact drug name, dose, timeline, and side effects
Visual symptoms, if any, such as blurry vision, field loss, eye pain, eyelid drooping, or double vision
Prior surgery or pathology records, if the patient already had a biopsy or operation
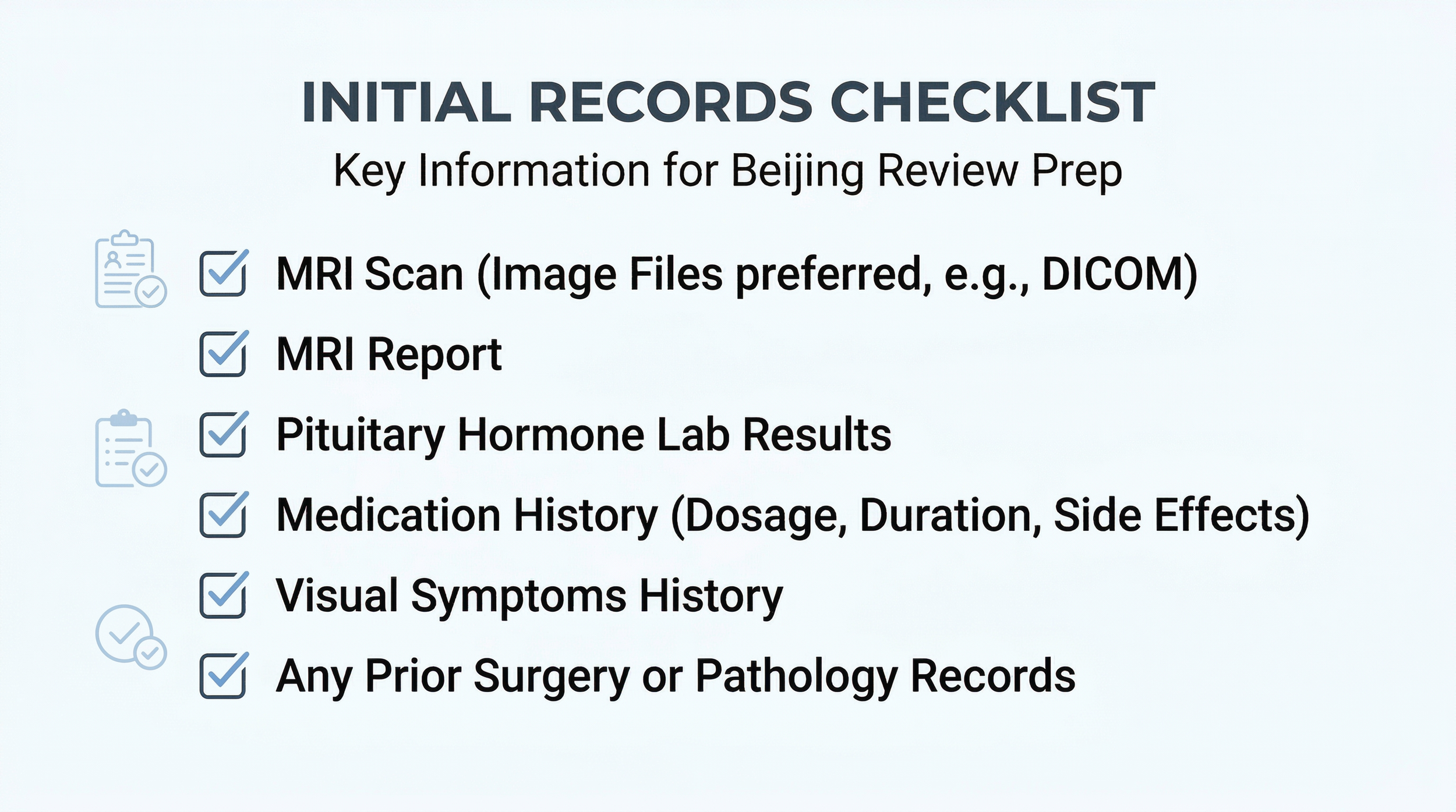
Figure 4 - Practical infographic checklist of medical records and patient data points often required for initial case organization and review with coordination teams.
Have old scans? That is often enough for an initial records check. You do not need to wait for a new MRI before asking what the next step usually looks like. If you are unsure which records matter most, email contact@pandamedglobal.com and ask what to prepare first.
If you are planning Beijing logistics with family
Medical decisions are only one part of the process. International patients also have practical questions: visas, lodging, translation, hospital registration, document formatting, and family travel timing.
If you are traveling with a spouse, parent, or other family member, or if you want to understand the basic coordination steps for treatment in Beijing, you can email contact@pandamedglobal.com and ask about records preparation, hospital process, and travel coordination details.
About the Author
Ryan Lee is a Beijing-based medical concierge and the founder of PandaMed. With a strict compliance background, he helps international patients navigate China's top public hospitals safely. He secures direct access to Chief Physicians for complex cases.
Medical Disclaimer
This information is for educational purposes only and is not medical advice. PandaMed is a care coordination service, not a medical provider. Always consult a qualified doctor for your specific condition.
References
Molitch ME. Diagnosis and Treatment of Pituitary Adenomas: A Review. JAMA. 2017;317(5):516-524. PubMed: https://pubmed.ncbi.nlm.nih.gov/28170483/
Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. PubMed search entry: https://pubmed.ncbi.nlm.nih.gov/
Reference: Pituitary surgical volume and joint-clinic pathway data, Peking Union Medical College Hospital, institutional public reporting and internal departmental summaries.
Reference: Neurosurgical and endoscopic skull base surgical volume data, Beijing Tiantan Hospital, institutional public reporting and specialty center summaries.