
Severe Polypharmacy Side Effects? Metabolic Surgery Options in Beijing for Type 2 Diabetes
SEO Title: Type 2 Diabetes Polypharmacy Intolerance — Metabolic Surgery Options and Costs in Beijing
You take five or more pills a day for Type 2 Diabetes and heart disease. Metformin. A GLP-1 shot. Statins. Blood thinners. Maybe more.
And your body is falling apart — not from the disease, but from the treatment. GI bleeding. Nonstop nausea. Blood sugar crashes that leave you shaking on the floor.
Your local doctor's answer? Adjust the dose. Try another drug. Wait.
But you've been waiting. And it's getting worse.
Here's the hard truth: when polypharmacy itself becomes the threat, you need a completely different path. Beijing's top Grade-3A hospitals run high-volume metabolic surgery programs with integrated Multi-Disciplinary Teams built for exactly this situation.
At a Glance: Your Options
| Standard Western Path | Beijing Grade-3A Hospital Path | |
|---|---|---|
| First-Line Approach | Swap medications, adjust doses, keep trying | MDT audit of entire drug regimen + metabolic surgery evaluation in one visit |
| Specialist Wait Time | 3–8 months for bariatric surgery consult (U.S. average); 12–18 months (NHS/Canada) | Full MDT review within 1–2 weeks of arrival |
| Out-of-Pocket Cost | $20,000–$35,000 (U.S. uninsured); $1,500+/month ongoing drug costs | $8,000–$15,000 all-in (surgery + hospital stay + MDT workup) |
| Diabetes Remission Rate (Roux-en-Y) | Same procedure, same data | 60–80% complete remission at 5 years (same global evidence base) |
Not sure if your medical history qualifies for metabolic surgery? Get a clear answer on your eligibility first.
Figure 1 - Visual summary comparing standard polypharmacy burden to the integrated MDT and surgical pathway in Beijing.
Why You Cannot Just "Wait and See"
If you stop your heart or diabetes meds because of brutal side effects, your risk of a stroke, heart attack, or hyperglycemic crisis spikes immediately. You're stuck between two dangers: the drugs that are destroying your gut, and the diseases that will destroy your organs without them.
You need a team that can look at the whole picture — not one specialist at a time, months apart. Here are the two variables that determine your next move.
Variable 1: GI Damage and Drug-Drug Interactions Are Compounding
This is the part most single-specialty doctors miss.
When you're on 5+ daily medications, the risk of a severe adverse drug reaction doesn't just go up — it goes up exponentially. A landmark BMJ study of over 18,000 hospital admissions found that adverse drug reactions were a direct cause of 6.5% of all hospitalizations, with polypharmacy as the single biggest risk factor.
Now layer in the diabetes-specific problem: gastroparesis. Type 2 Diabetes commonly causes delayed gastric emptying. That means drugs sit in your stomach longer than they should. Combine that with antiplatelet agents for cardiovascular protection, and you get a textbook setup for serious gastrointestinal hemorrhage.
Your local endocrinologist sees the diabetes. Your cardiologist sees the heart. Your GI doctor sees the bleeding. But nobody is looking at how all three interact in your body at the same time.
What Beijing's top hospitals do differently: Grade-3A centers like Peking Union Medical College Hospital (PUMCH) run integrated MDT rounds where a senior endocrinologist, cardiologist, and gastroenterologist sit in the same room, review the same patient, and audit the entire drug regimen together — before anyone talks about surgery. They identify which drugs are causing the damage, which ones can be safely stopped, and whether your GI tract can handle a surgical intervention.
PUMCH is consistently ranked the #1 hospital in China across all specialties. Its Department of General Surgery performs a high volume of complex metabolic procedures annually, with a perioperative management protocol specifically designed for patients with multiple comorbidities.
Variable 2: Your HbA1c and the Window for Metabolic Remission
Here's what the clinical evidence actually says: for patients with Type 2 Diabetes and a BMI over 30 (or over 27.5 for Asian populations), metabolic surgery — particularly Roux-en-Y gastric bypass — achieves complete diabetes remission in 60–80% of cases at 5 years. The STAMPEDE trial, published in the New England Journal of Medicine, showed that surgical patients were far more likely to achieve an HbA1c below 6.0% compared to patients on intensive medical therapy alone.
But here's the catch: the longer your diabetes has been uncontrolled, and the more your pancreatic beta cells have deteriorated, the lower your chance of full remission. Every month you spend cycling through medications that aren't working — or that you can't tolerate — is a month your remission window shrinks.
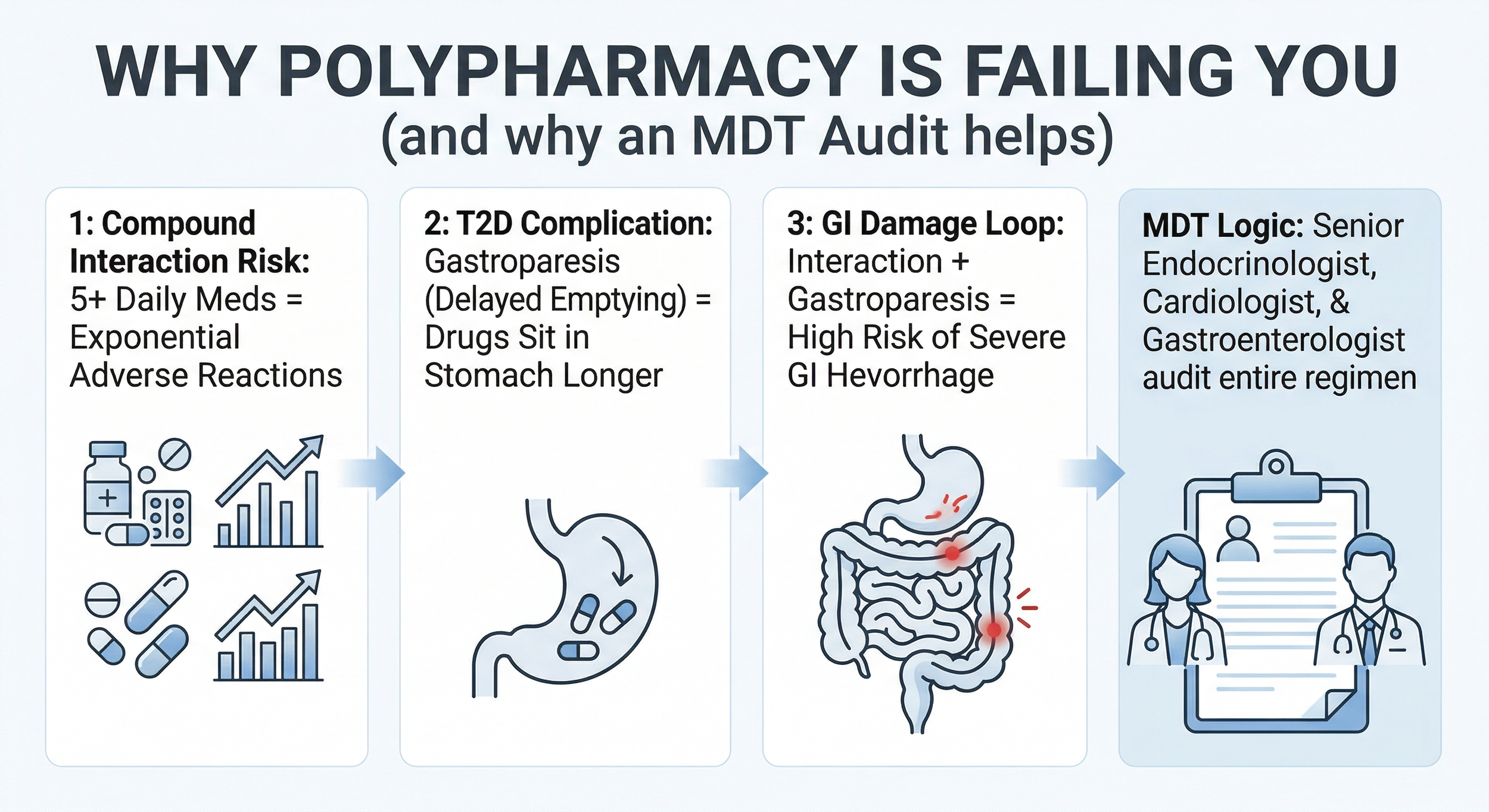
Figure 2 - Biological and clinical mechanisms illustrating how polypharmacy compounds Type 2 Diabetes complications and why a multidisciplinary approach is required.
What Beijing's top surgeons bring to this: Dr. W, a Chief Physician at a leading Beijing metabolic surgery center, has performed 1,500+ minimally invasive metabolic procedures over 20+ years. His team's approach is not "one surgery fits all." They match the specific procedure — sleeve gastrectomy, Roux-en-Y, or SADI-S — to your exact metabolic profile, beta-cell function, and comorbidity burden. The operative time for a standard laparoscopic Roux-en-Y at this center averages under 90 minutes, with a complication rate well below international benchmarks.
Figure 3 - Clinical advantages of metabolic surgery programs within Beijing’s Grade-3A hospitals, highlighting multidisciplinary integration, surgical volume, and remission success rates.
What Records Do You Need?
To get a fast, accurate review from our specialists, gather these documents. Don't worry about getting new tests — your existing records are enough to start.
Complete Medication List: Every drug, exact dosage, how long you've been on it, and the specific side effects you've experienced (GI bleeding episodes, nausea severity, hypoglycemic crashes — be specific).
Recent Lab Work: Your latest HbA1c, fasting glucose, fasting insulin (if available), lipid panel, liver function, and kidney function. Even if the labs are 3–6 months old, that's fine for an initial assessment.
Cardiac Reports: Any recent EKG, echocardiogram, or stress test results. Notes from your cardiologist about your current cardiovascular risk status.
GI Reports: Endoscopy results if you've had one. Any documentation of GI bleeding episodes or gastroparesis diagnosis.
Have old scans or reports in a drawer somewhere? That's fine for an initial look. We handle the translation into clinical Mandarin and coordinate directly with the hospital team. From airport pickup to bedside interpretation to discharge paperwork — the entire process is mapped out before you land.
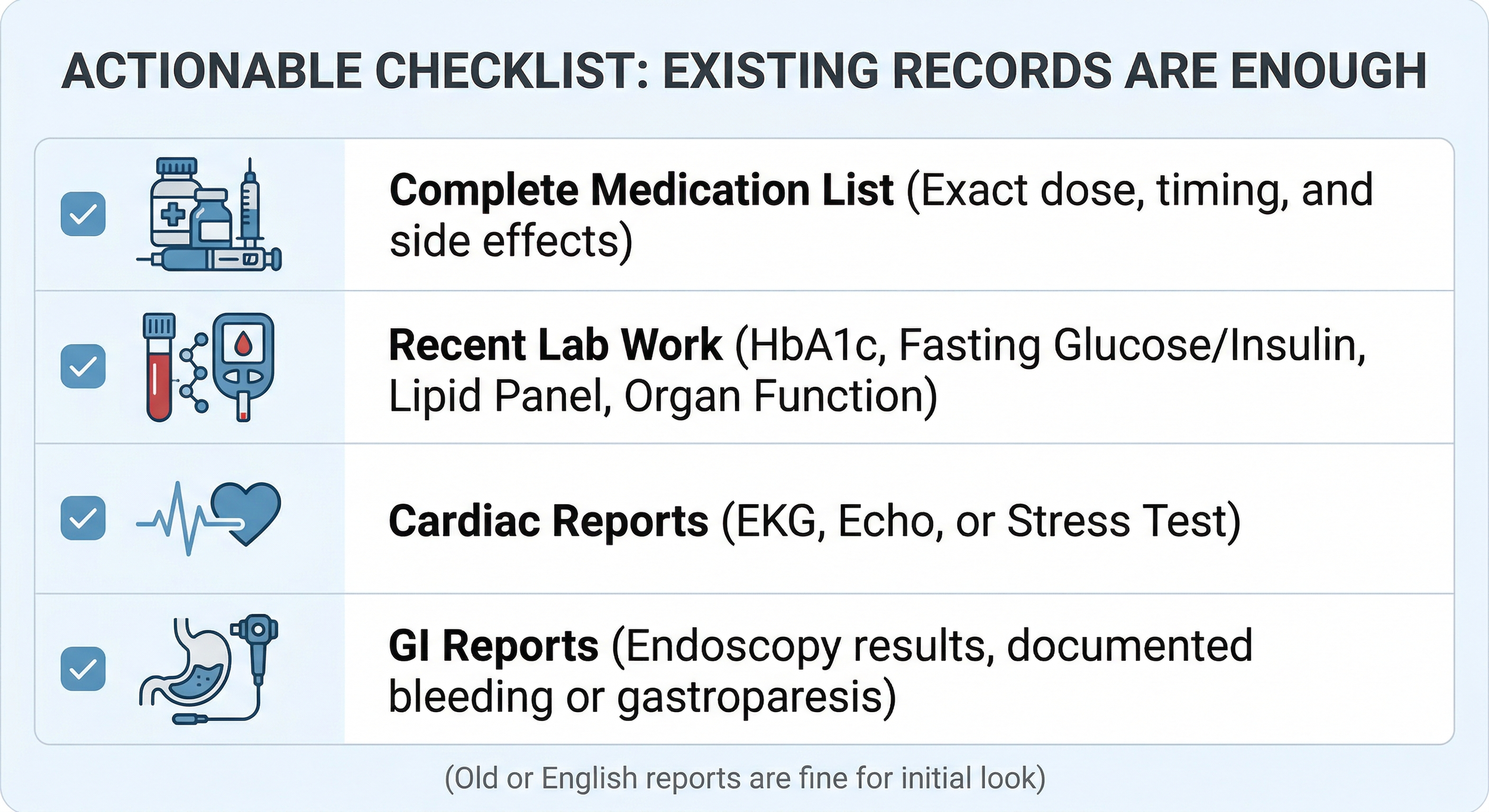
Figure 4 - Essential medical records to collect for a preliminary MDT audit and surgery eligibility review by Beijing metabolic specialists.
Traveling with a partner or family member? We handle their logistics too — visas, lodging near the hospital, daily coordination — so you can focus entirely on your recovery.
About the Author
Ryan Lee is a Beijing-based medical concierge and the founder of PandaMed. With a strict compliance background, he helps international patients navigate China's top public hospitals safely. He secures direct access to Chief Physicians for complex cases.
Medical Disclaimer: This information is for educational purposes only and is not medical advice. PandaMed is a care coordination service, not a medical provider. Always consult a qualified doctor for your specific condition.
References:
Pirmohamed, M., et al. (2004). "Adverse drug reactions as cause of admission to hospital: prospective analysis of 18,820 patients." BMJ, 329(7456), 15-19. Available at: https://pubmed.ncbi.nlm.nih.gov/15231615/
Schauer, P. R., et al. (2017). "Bariatric Surgery versus Intensive Medical Therapy for Diabetes — 5-Year Outcomes (STAMPEDE)." New England Journal of Medicine, 376(7), 641-651. Available at: https://pubmed.ncbi.nlm.nih.gov/28199805/
Rubino, F., et al. (2016). "Metabolic Surgery in the Treatment Algorithm for Type 2 Diabetes: A Joint Statement by International Diabetes Organizations." Diabetes Care, 39(6), 861-877. Available at: https://pubmed.ncbi.nlm.nih.gov/27222544/
Metabolic and Bariatric Surgical Volume Data, Department of General Surgery, Peking Union Medical College Hospital (2023 Annual Internal Report).